Prof. Dr. Konstantin Nikolaou is, on paper, one of the best-positioned people in European radiology to talk about this. Chairman of the Department of Diagnostic and Interventional Radiology at the University of Tübingen, in Tübingen, Germany. vice-president of the German Röntgen Society (DRG). Chair of the European Society of Radiology (ESR)'s first statutory AI and Digital Technologies Committee.
Making innovation trustworthy
The EU AI Act is already in force. AI literacy obligations already apply. Nikolaou walked through what that actually means on a Tuesday morning in a German radiology department.
 Prof. Dr. Konstantin Nikolaou, chairman of the Department of Diagnostic and Interventional Radiology at the University of Tübingen, and chair of the ESR's AI and Digital Technologies Committee is one of the most influential voices on AI governance in European radiology.
Prof. Dr. Konstantin Nikolaou, chairman of the Department of Diagnostic and Interventional Radiology at the University of Tübingen, and chair of the ESR's AI and Digital Technologies Committee is one of the most influential voices on AI governance in European radiology.
"The AI Act is not anti-innovation," he noted. "It is a framework to make innovation trustworthy."
That is partly the point of the ESR's new statutory committee. Not an advisory group. A permanent mandate, defined responsibilities, and a seat in the formal governance structure of the society, with direct lines to regulators, industry partners, and other ESR bodies. The move from working group to statutory committee reflects that AI is no longer peripheral to radiology -- it is structural, noted Nikolaou.
Leading, not reacting
"Radiology should not wait passively for regulation," Nikolaou said. "We should help define how safe, clinically useful AI is implemented in real patient care." The field has spent years watching AI get defined around it. The committee exists, in part, to change that dynamic.
What he also flagged, and what often gets lost in the governance conversation, is the monitoring layer. Once an AI system is embedded in clinical practice, it needs continuous oversight. Performance can drift, patient populations shift, imaging equipment changes. The deployment moment is not the finish line. It is closer to the starting gun.
The infrastructure question
The European Health Data Space (EHDS) is a topic where the gap between ambition and reality is worth examining closely.
Germany is not starting from zero. The Netzwerk Universitätsmedizin (NUM) initiative and, within it, the RACOON project, the Radiology Cooperative Network, have already built federated data infrastructure that moves meaningfully toward the interoperability and governance standards EHDS will require. Secure, multicenter data sharing for research has been demonstrated in practice. Not in a pilot. In a functioning network.
That matters in a European landscape where EHDS implementation is uneven and the gap between member-state readiness varies considerably. Germany has infrastructure that other countries are still building toward.
But challenges remain. Interoperability between heterogeneous hospital IT systems is still inconsistent. The pace of implementation across Germany is slower than the ambition suggests. The distance between what RACOON has proved possible and what a community hospital in a smaller city can actually do with its data remains significant.
Radiology has been one of medicine's most consistently digital specialties for decades. That history is an asset as the field is better placed than most to help shape what European health data integration looks like in practice, rather than inherit a framework built without imaging departments at the table.
Whether that positioning translates into actual influence over EHDS implementation, at the member state level, at the hospital IT procurement level, at the level of the radiologist who needs the data to actually be usable, is a different and still open question.
When evidence meets reality
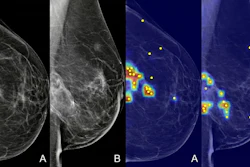
Reimbursement is a systemic problem in German radiology. Prostate cancer imaging is one of the clearest examples.
Multiparametric MRI (mpMRI) for prostate cancer is in current German guidelines. The clinical evidence is strong, long-established, and not in dispute. The exam is already used widely in routine patient care across Germany. Demand is high. Specialist radiologists trained in prostate MRI interpretation exist. Yet the reimbursement still hasn't caught up.
"We face a paradox," Nikolaou said. "The evidence is clear, the clinical demand is high, but sustainable financing and nationwide access are still insufficiently regulated."
He was careful about what AI can actually fix here. It can support workflow efficiency. It can improve consistency in settings where specialist expertise is limited. It can help scale access in ways that a shortage of expert readers alone cannot. "AI can help us scale expertise," he said, "but it cannot replace well-trained radiologists or necessary healthcare policy decisions or infrastructure development."
The technology is available, the trained professionals exist and the clinical case has been made, repeatedly, in peer-reviewed literature and in national guidelines. What remains is a structural decision that no algorithm can substitute for.
There is movement. The Gemeinsamer Bundesausschuss (G-BA), Germany's Federal Joint Committee, has opened a formal evaluation process for organized prostate cancer screening, including PSA-based population screening pathways combined with MRI. If organized screening is implemented, demand for high-quality prostate MRI across Germany could rise substantially, and quickly.
That makes the reimbursement question more urgent, not less. If screening rolls out and the payment structures still haven't caught up, the bottleneck moves from evidence to logistics to finance, and patients wait at each stage.
The clinical case closed a while ago. The policy case is still being written.
Our full coverage of RöKo 2026 can be found here.