LEIPZIG - Lung cancer kills more Europeans than any other cancer. Not because it is untreatable, but because it is almost always caught too late.
At RöKo 2026 in Leipzig, a highlight session on interdisciplinary early detection took stock of where Germany stands six weeks into its national low-dose CT (LDCT) screening program, and what is still not working.
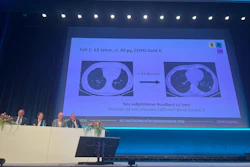
 Early-stage findings are not always straightforward, and multidisciplinary judgment is not a formality, the nodule conference at the close of the highlight session "Us against lung cancer" made that clear. RöKo 2026, Leipzig.Claudia Tschabuschnig
Early-stage findings are not always straightforward, and multidisciplinary judgment is not a formality, the nodule conference at the close of the highlight session "Us against lung cancer" made that clear. RöKo 2026, Leipzig.Claudia Tschabuschnig
The formal launch was on 1 April 2026, when LDCT screening became a statutory benefit under Germany's national health insurance system. The program targets adults ages 50 to 75 with a significant smoking history -- at least 20 pack-years, current smokers or those who quit within the past 10 years. First readings bill at €49.56, while the specialized second read at a certified lung cancer center bills at €95.04.
The gap between policy and practice opened almost immediately. Health insurers refused to reimburse the digital platform infrastructure required to manage double-reading workflows.
"The health insurance providers have said: a platform like this is not provided for in the guidelines, and if it is not provided for, it will not be paid for," Markus Henkel, BDR managing director and legal counsel, said at that session.
"The first of April was a virtual start date," Dr. Jörg Barkhausen of Universitätsklinikum Schleswig-Holstein in Lübeck, Germany, said: A few administrative steps, he noted, still need time.
The evidence holds
Lung cancer remains Germany's deadliest malignancy, with approximately 45,000 deaths annually. Only around 15% of cases are caught at stage I. More than half present at stage IV, when treatment options are severely limited.
The German HANSE study, published in Lancet Oncology in November 2025, screened more than 5,000 participants twice with low-dose CT. Of 111 carcinomas detected across roughly 10,000 examinations, 85 -- more than three-quarters -- were at stage I or II. Five-year survival in early-stage disease exceeds 70%. In stage IVb, 7% of patients are alive after five years.
Dr. Torsten Bauer of Lungenklinik Heckeshorn in Berlin addressed skepticism directly. A newsletter from the Bundesverband der Pneumologen had suggested randomized trials show no clear benefit in overall mortality. Bauer pushed back, presenting meta-analyzed data showing consistent reduction in lung cancer-specific mortality. Overall mortality moves more slowly, he acknowledged.
What happens after the referral
Every scan requires a first read and a second read, the second mandated at a certified lung cancer center. Findings classified as Lung-RADS 3 or higher trigger the secondary read workflow. Discordant findings trigger a nodule conference. Certified centers cannot simply bill without first obtaining a formal exemption from restrictions that normally apply to hospital-based specialists in outpatient care, a process that runs through regional licensing committees.
Seven years of work across radiology, pulmonology, and thoracic surgery brought Germany to 1 April. Prof. Dr. Johannes Wessling of Universitätsklinikum Münster in Münster, Germany, presented the Münsterland initiative, a regional platform connecting referring physicians, first readers, and lung cancer centers on a single digital infrastructure: automated screening IDs, digital consent, real-time dashboards, direct appointment booking.
His presentation carried a structural warning: digital gaps and paper-based handoffs do not just slow the process. They cost participants. And lost participants mean undetected cancers.
"We lose participants at every interface," Wessling said.
The Münsterland model covers 1.6 million inhabitants, with a target population of around 105,000 eligible individuals. At realistic participation rates, Wessling estimated a maximum of around 42 CT screenings per day for participating centers -- a manageable volume, but only if the logistics hold.
Regional cooperation models like this are beginning to emerge as a practical response to the infrastructure gap. The state radiology association in Bremen is coordinating three lung centers with all regional radiologists, a structure Prof. Dr. Hermann Helmberger, BDR president, highlighted at RöKo Digital as a replicable template.
AI is mandatory, quality is not
AI-assisted software for nodule detection is not optional in this program -- it is mandated. What remains unresolved is quality. CE certification, as Barkhausen noted, is a market-entry label, not a performance guarantee. Certified systems can differ meaningfully in what they detect. Standardized performance criteria for screening-specific AI do not yet exist.
The interoperability problem compounds this. Until RIS vendors implement proper digital referral workflows, practices risk managing patient handoffs manually between first and second readers running different systems, including AI tools from different vendors that may not process prior imaging acquired under nonstandard protocols.
The surgical side
Dr. Katrin Welcker of Helios Klinikum Mönchengladbach in Mönchengladbach, Germany, focused on the clinical stakes. Small and centrally located tumors require close radiological-surgical coordination -- CT-guided marking before resection, robotic-assisted approaches where needed.
The nodule conference cases presented at the end of the session illustrated the reality: early-stage findings are not always straightforward, and multidisciplinary judgment is not a formality.
Our full coverage of RöKo 2026 can be found here.