CT is the best tool for identifying pelvic fractures and active hemorrhage, and rapid detection, localization, and characterization of a vascular injury on CT helps to stratify the treatment of patients and guide interventional radiologists to perform targeted arteriography, according to prizewinning research from Madrid.
"The ability to characterize arterial injuries and to differentiate them from venous injuries is important for ensuring appropriate and timely treatment," noted Dr. Silvia Cayón Somacarrera, radiologist at Hospital Universitario de La Princesa, and colleagues.
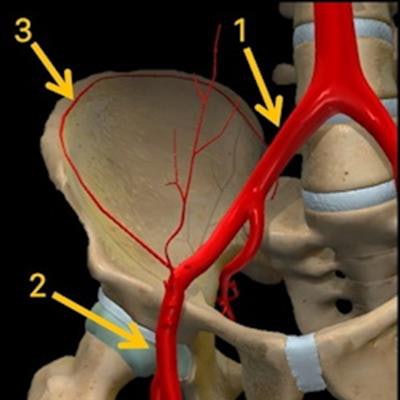
 Anatomy of external iliac artery (1), femoral artery (2), and deep circumflex iliac artery (3). All figures courtesy of Dr. Silvia Cayón Somacarrera and colleagues, presented at ECR 2022.
Anatomy of external iliac artery (1), femoral artery (2), and deep circumflex iliac artery (3). All figures courtesy of Dr. Silvia Cayón Somacarrera and colleagues, presented at ECR 2022."Familiarity with the anatomy of the pelvic vessels is helpful in identifying and localizing the source of bleeding. Tracing the bleeding vessel is not always possible using CT, and utilisation of vascular territories allows for rapid identification of the most likely bleeding vessel," they stated in an e-poster presentation that received a magna cum laude award at ECR 2022.
The aim of the exhibit -- called "Bloody hell: Who is the bleeder?" -- was to give easy tips to determine on CT the most probable bleeding artery in pelvic hemorrhages based on a map that shows an approximation of the zonal pelvic vascularization.
Vascular pelvic injuries are the major cause of morbidity and mortality in blunt trauma patients, the authors explained. Historically, they have been evaluated with arteriography, but CT enables a rapid noninvasive evaluation, making it possible to differentiate between arterial and venous bleeding, which is a key factor when considering the most suitable treatment.
"In active bleeds, determining whether the bleeding is arterial (high pressure bleeding) or venous (low pressure bleeding) is important," they pointed out. "Once we have identified there is an arterial active bleeding and we have determined its location, knowing the zonal pelvic vascularization map can help us determine the most probable bleeding artery."
In general, these findings correlate with those found later in arteriography, but around 20%-40% of patients who did not show active arterial bleeding on CT had it on arteriography. This could be due to intermittent bleeding secondary to arterial spasm or temporary tamponade by the hematoma itself, the researchers said.
Procedure details
First of all, it is vital to differentiate between the various types of active bleeding. Arterial bleeding is depicted as a contrast extravasation in the arterial phase that increases in the successive phases (portal and delayed phases), while venous bleeding is shown as a contrast extravasation in the portal phase that increases in the delayed phase (absence of bleeding in the arterial phase).
"It is also important to know the findings that allow us to determine the existence of a pseudoaneurysm," they added. "It manifests as a hyperdense focal zone in the arterial phase with progressive washout in successive phases (portal and delayed phases)."
 Bilateral femoral artery pseudoaneurysm following aortobifemoral bypass surgery. Pseudoaneurysms constitute an uncommon complication (less than 3% of patients) of aortic reconstructive surgery. They result from partial or total disruption of the anastomosis between an artery and a vascular graft, creating a pulsatile hematoma with fibrous encapsulation. The femoral artery is the most common site involved, accounting for about 75% of cases, and it usually occurs around the anastomotic site of the femoral bypass.
Bilateral femoral artery pseudoaneurysm following aortobifemoral bypass surgery. Pseudoaneurysms constitute an uncommon complication (less than 3% of patients) of aortic reconstructive surgery. They result from partial or total disruption of the anastomosis between an artery and a vascular graft, creating a pulsatile hematoma with fibrous encapsulation. The femoral artery is the most common site involved, accounting for about 75% of cases, and it usually occurs around the anastomotic site of the femoral bypass.In the ECR 2022 poster, the researchers gave examples of arterial pelvic lesions, including active bleeds and pseudoaneurysms, located in the different vascular zones.
In the abdominal aorta, there are five pairs of lumbar arteries, they explained. The first two pairs are direct branches of the abdominal aorta and the fifth pair is a branch of the middle sacral artery. They supply the muscles of the posterior abdominal wall, lumbar vertebrae, spinal cord, and meninges.
The median sacral artery arises from the iliac bifurcation and supplies the L4 and L5 vertebrae and the sacrum, while the inferior epigastric artery arises from the external iliac artery and ascends to supply the rectus abdominis muscle, anastomosing with the superior epigastric artery, which is a branch of the internal mammary artery.
The common iliac artery bifurcates into the internal and the external iliac arteries, the authors wrote. After traveling under the inguinal ligament, the external iliac artery becomes the common femoral artery. The external iliac artery gives off two branches: the inferior epigastric artery and the deep circumflex iliac artery, and the latter supplies the muscles of the anterolateral abdominal wall.
In the internal iliac artery, it is essential to keep aware of the anterior trunk, particularly the obturator artery (which supplies the external obturator muscle and the hip adductors), the inferior gluteal artery (which supplies gluteus maximus, piriformis, internal obturator, superior and inferior gemelli, and quadratus femoris muscles), and the internal pudendal artery (which supplies the muscles of anal and urogenital region), they added.
In the posterior trunk of the internal iliac artery, the following are important: the iliolumbar artery (which supplies psoas major, quadratus lumborum and iliacus muscles), lateral sacral artery (which supplies the erector spinae and piriformis muscles, and the sacrum), and the superior gluteal artery (which supplies piriformis, internal obturator, gluteus maximus, medius and minimus, and tensor fasciae latae muscles).
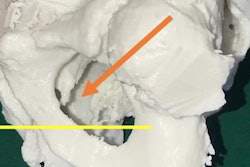
 Active bleeding in the lateral sacral artery.
Active bleeding in the lateral sacral artery."We should also be aware of a common anatomic variant called the corona mortis which is present in up to 30% of patients. It is an aberrant anastomotic connection between the obturator artery and the inferior epigastric artery," the authors noted.
This must be considered as a source of bleeding if the internal iliac arteriography does not reveal a pelvic source of the bleeding, and in such instances, arteriography of the external iliac artery should be performed to exclude bleeding from the corona mortis, they stated.
The other authors of the award-winning ECR 2022 e-poster were Dr. María Cristina Iniesta González and Dr. Alberto Mingo Basail, both from Hospital Universitario de La Princesa in Madrid; María Luz Parra Gordo, PhD, from Hospital Universitario de La Paz in Madrid; and Dr. Itxaso Galán González, from Hospital Universitario Infanta Leonor in Madrid.
 Dr. Silvia Cayón Somacarrera attended ECR 2022, and now works as a musculoskeletal radiologist at Marqués de Valdecilla University Hospital, Cantabria, Spain.
Dr. Silvia Cayón Somacarrera attended ECR 2022, and now works as a musculoskeletal radiologist at Marqués de Valdecilla University Hospital, Cantabria, Spain.You can view the full ECR exhibit on the EPOS section of the European Society of Radiology website.