
LIVERPOOL -- Certain B3 lesion types and imaging characteristics have a higher risk of upgrading to a cancer within three years and should be considered for more regular screening. That's the view of researchers from a top London hospital who presented the results of a new 10-year study at the U.K. Imaging and Oncology Congress (UKIO).
Breast lesions classified as being of uncertain malignant potential (B3) are a diverse group of abnormalities with a variable but low risk of associated malignancy and borderline histological spectrum, according to Olivia Taylor-Fry, consultant radiographer at St. George's University Hospitals NHS Foundation Trust, and colleagues. At the time of diagnosis, these lesions coexist with an adjacent malignancy or suggest an increased risk of developing a future malignancy.
 Mammogram with grouped heterogeneous microcalcifications showing linear distribution attributable to atypical ductal hyperplasia.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
Mammogram with grouped heterogeneous microcalcifications showing linear distribution attributable to atypical ductal hyperplasia.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
B3 lesions are challenging to categorize histologically, requiring specialist training and multidisciplinary input, according to the authors of these guidelines. "They may coexist with in situ or invasive breast cancer (BC) and increase the risk of subsequent BC development. Management should focus on adequate classification and management whilst avoiding overtreatment."
The U.K. landscape
B3 breast lesions account for 6.7% (range 3.3% to 12.6%) of all core biopsies performed in the U.K. National Health Service (NHS) Breast Screening Programme, noted Taylor-Fry, who is also a PhD student at the University of Salford. Positive predictive values range from 14 to 28%, depending on the specific type of B3 lesion. Advances in imaging technology and enhanced screening programs appear to be contributing to the rising incidence of B3 lesions across Europe.
In the U.K., 2016 guidance recommended vacuum-assisted or surgical excision of B3 lesions, followed by yearly breast imaging surveillance for five years. In 2025, new guidelines stated that annual surveillance of these patients may not be necessary and suggested returning these women to regular screening every three years.
 Amorphous microcalcifications with a segmental distribution typical of lobular neoplasia.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
Amorphous microcalcifications with a segmental distribution typical of lobular neoplasia.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
A total of 1,504 patients were diagnosed with a B3 breast lesion over this period, of which 1,346 were new B3 diagnoses with no history of breast cancer. Of these cases, 308 (23%) were upgraded to a cancer (B5a/B5b) at subsequent vacuum excision/surgical excision. In treatment, 934 VAEs were performed, along with 412 surgical excisions. From the total, 1,038 cases remained benign and had subsequent five-year follow-up imaging.
The team identified 17 upgrades (1%) into cancer within the zero- to three-year follow-up period. Of these, 11 (65%) were cases of B3 atypical intraductal epithelial proliferation (AIDEP), which has the highest upgrade rate to a cancer. 55% of the AIDEP cases upgraded into invasive cancer.
 Grouped coarse heterogeneous microcalcifications.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
Grouped coarse heterogeneous microcalcifications.Dr. Isabel T. Rubio et al, European Journal of Surgical Oncology
"This study showed that cases of AIDEP and in situ lobular neoplasia had the highest upgrade to malignancy within the 0-3-year period," the authors pointed out.
Calcifications are most commonly detected at screening mammography and found incidentally in symptomatic patients, giving no symptoms and not being clinically palpable.
"The ability of AIDEP cases to progress to ductal carcinoma in situ or invasive carcinoma is unpredictable," they continued. "Multidisciplinary and concordant imaging and pathology discussions are crucial to ensure this cohort of patients are followed up effectively."




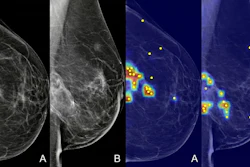











![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnieeurope.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)
