Breast MRI is becoming increasingly valuable in the management of patients with suspicious nipple discharge and a negative mammogram and ultrasound scan, a new French study has shown.
"In patients with suspicious nipple discharge and normal mammogram and ultrasound, MRI demonstrates excellent performance to identify lesions for which excision is required," reported Dr. Martine Boisserie-Lacroix and colleagues from the radiology department at Bergonié Institute Comprehensive Cancer Centre in Bordeaux, France. "Normal MRI indicates it is safe to propose follow-up only management, thus avoiding unnecessary duct excision."
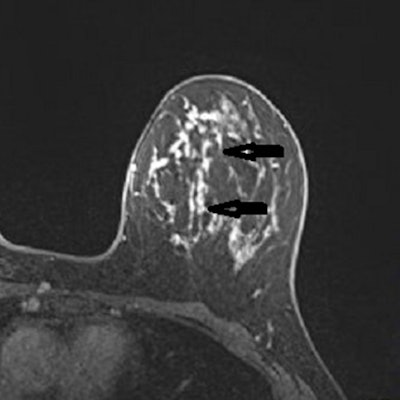
 A 53-year-old woman with previous right mastectomy and uniporous left bloody discharge. Above: MRI axial plane after injection with fat saturation shows a left nonmass enhancement with linear distribution in the inner inferior quadrant (arrow). Below: Second-look ultrasound demonstrates three ducts of normal caliber in correlation (arrow). 10-G vacuum-assisted biopsy under ultrasound guidance revealed papilloma removed by surgical excision. Images courtesy of Dr. Martine Boisserie-Lacroix and European Radiology.
A 53-year-old woman with previous right mastectomy and uniporous left bloody discharge. Above: MRI axial plane after injection with fat saturation shows a left nonmass enhancement with linear distribution in the inner inferior quadrant (arrow). Below: Second-look ultrasound demonstrates three ducts of normal caliber in correlation (arrow). 10-G vacuum-assisted biopsy under ultrasound guidance revealed papilloma removed by surgical excision. Images courtesy of Dr. Martine Boisserie-Lacroix and European Radiology.MRI detected a lesion requiring excision in 46 participants (45%) with unexplained discharge, and if a breast MRI scan is negative, follow-up is a safe alternative for these patients, the authors wrote in an article published on 13 April in European Radiology.
Evolution of MRI's role
In the early 2000s, some researchers investigated MRI's potential in patients with nipple discharge, and since then, several studies have emphasized the role of MRI as an alternative to galactography in patients with inconclusive findings on conventional imaging.
"While MRI is recommended by several guidelines, these studies have investigated the diagnostic utility of MRI in the detection of malignant lesions only. Their limitations are the mainly retrospective nature and the variety of inclusion criteria (pathological and physiological discharge, exclusively bloody discharge or any kind of discharge, normal and abnormal findings at conventional imaging)," they noted. "Additional data are therefore needed to confirm the role of breast MRI in this indication."
The authors' aim was to evaluate the diagnostic accuracy of breast MRI in identifying lesions requiring excision for patients who had experienced suspicious nipple discharge but had normal mammograms and ultrasound scans.
Between September 2013 and May 2019, 106 women (mean age, 57.9 years) were consecutively included in this prospective multicenter study, with 102 being retained for analysis. MRI was considered negative in the absence of suspicious enhancement and positive in cases of ipsilateral abnormal enhancement (BI-RADS 3 to 5). Final diagnoses were based on histological findings of surgical or percutaneous biopsies or at one-year follow-up.
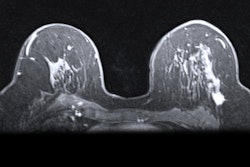
 MRI axial plane after injection with fat saturation (above, arrows) and subtraction (below) shows a large nonmass micronodular enhancement with segmental distribution in the inner left quadrants. Mastectomy: 130-mm ductal carcinoma in situ with microinvasion. Images courtesy of Dr. Martine Boisserie-Lacroix and European Radiology.
MRI axial plane after injection with fat saturation (above, arrows) and subtraction (below) shows a large nonmass micronodular enhancement with segmental distribution in the inner left quadrants. Mastectomy: 130-mm ductal carcinoma in situ with microinvasion. Images courtesy of Dr. Martine Boisserie-Lacroix and European Radiology.The authors considered all lesions requiring excision found on pathology (papilloma, atypia, nipple adenomatosis, or cancer) as positive results, and they viewed spontaneous resolution of the discharge at one year as a negative result.
MRI showed ipsilateral abnormal enhancement in 54 patients (53%), revealing 46 lesions requiring excision (31 benign papillomas, five papillomas with atypia, two nipple adenomatosis, and eight cancers) and eight benign lesions not requiring excision. The team found no suspicious enhancement in the remaining 48 women (47%). Forty-two were followed up at one year with spontaneous resolution of the discharge, and six underwent surgery (revealing two benign papillomas).
 Dr. Martine Boisserie-Lacroix. Image courtesy of the Bergonié Institute.
Dr. Martine Boisserie-Lacroix. Image courtesy of the Bergonié Institute.Overall, MRI diagnostic accuracy for the detection of a lesion requiring excision was 96% sensitivity, 85% specificity, 85% positive predictive value, and 96% negative predictive value.
"Given the excellent sensitivity and negative predictive value for detecting a lesion requiring excision, these results indicate that pyramidectomy may be unnecessary in MRI-negative patients where spontaneous resolution of nipple discharge was observed in most cases," Boisserie-Lacroix and colleagues stated. "The clinical and imaging follow-up for one year or more seems a safe alternative."
These results should lead to the development of standardized guidelines for this patient group for whom very little prospective imaging data existed, they concluded.
"Our results were not surprising as the study confirmed our daily care, but we needed academic confirmation," Boisserie-Lacroix told AuntMinnieEurope.com on 16 April, adding that she hopes this approach to patient management will be accepted by all radiologists and confirmed in guidelines.
The Bordeaux group is not currently working on any follow-up studies, but Boisserie-Lacroix and her colleagues intend to maintain their long-term interest in the topic.