A recent study published in EANM Innovation put numbers on a problem nuclear medicine professionals have long recognized but rarely quantified: the gap between what international PET/CT guidelines recommend and what actually happens in clinical practice.
Researchers at University Hospital Bonn in Germany systematically compared European Association of Nuclear Medicine (EANM) and Society for Nuclear Medicine and Molecular Imaging (SNMMI) guidelines against their own institutional standard operating procedures (SOP) for three widely used PET/CT protocols -- FDG, PSMA, and DOTATOC -- using a structured framework they call the "Action Corridor" model.
The framework categorizes each parameter as conforming to guidelines, a justified local adaptation, a specification of a generic recommendation, or a potential inconsistency requiring review.
The most notable finding involved DOTATOC imaging for neuroendocrine tumors. Institutional practice applied an uptake time of 30 minutes, against a guideline-recommended window of 55 to 90 minutes, with a practice-to-guideline ratio of 0.41. The authors describe this as the most pronounced deviation across all three protocols and note that early imaging at 30 minutes may underestimate tracer uptake and reduce quantitative comparability, given the kinetic characteristics of somatostatin receptor ligands. The department revised its DOTATOC SOP in response to the study.
Across protocols, institutional practice consistently used shorter uptake times. For PSMA PET/CT, institutional practice used 45 minutes against a guideline target of approximately 60 minutes. For FDG oncology imaging, the same 45-minute uptake time was recorded against a recommended 60-minute target, and the permissible blood glucose threshold was set at less than 200 mg/dL against the guideline's less than 140 mg/dL, a ratio of 1.43. Both deviations were classified as potential inconsistencies.
Why comparability matters
The authors note that uptake time variations of 10 to 15 minutes around the 60-minute FDG reference are associated with SUV changes in the range of approximately 5% to 15%, depending on tumor biology. This has implications for multicenter comparability.
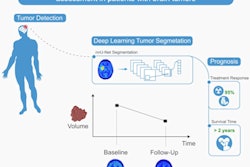
The clinical stakes of that comparability problem are concrete. PET/CT is increasingly used not just to detect lesions but to measure whether a tumor responds to treatment, based on quantitative SUV values. If a patient's baseline scan is acquired at 60 minutes and a follow-up scan at 30 minutes due to a local protocol deviation, the numbers may suggest tumor change that does not reflect biological reality. The concern is less about isolated scans than the gradual accumulation of local workflow adaptations that reduce reproducibility over time.
However, not all deviations were negative. Radiation exposure for FDG was measurably lower in practice than the guideline reference value, reflecting dose optimization through modern scanner technology and reconstruction techniques, classified as a justified adaptation.
Why gaps persist
Lead author Oleg Obolenski, MSc, of the department of nuclear medicine at University Hospital Bonn, emphasized that the findings should not be read as a critique of individual centers.
"These gaps usually do not persist because guidelines are unknown or ignored," he told AuntMinnieEurope. "In routine clinical workflows, the challenge is that guideline recommendations must be translated into local SOPs, scanner-specific protocols, staffing models, patient logistics, and daily operational realities."
In the Bonn case, a major PET/CT infrastructure modernization, including installation of a fully digital PET/CT system and substantial workflow restructuring, contributed to the deviations.
"Such technological transitions often improve image quality, reduce radiation exposure, and increase throughput, but they may also lead to local workflow adaptations that persist over time if SOPs are not continuously reevaluated against updated international recommendations," Obolenski said.
A further structural challenge is that SOPs are typically maintained as complex free-text documents updated through multiple local processes.
"Over time, practical workflow adaptations can become embedded in routine clinical practice without systematic reharmonization," he noted.
Clinical implications
The study does not demonstrate direct diagnostic errors caused by shortened uptake times, and Obolenski was careful about the limits of what could be concluded.
"Uptake time is considered a highly relevant parameter in PET imaging because it directly influences tracer biodistribution and quantitative measurements such as SUV values," he said. "Variations in uptake time can therefore affect the comparability between examinations, between scanners, and potentially between institutions."
The concern, he added, is less about isolated individual scans and more about the cumulative effects of standardization.
"This becomes particularly important in longitudinal follow-up, therapy monitoring, multicenter studies, and theranostic decision-making, where reproducibility and harmonization are essential."
The AI component
The study also assessed whether generative AI could reliably extract procedural parameters from unstructured SOP documents for quality auditing. Using GPT-5, the researchers extracted 21 predefined quantitative parameters across the three protocols from institutional SOPs written in German and English. After independent human verification, no discrepancies were found.
Large hospital departments may maintain extensive SOP documentation that is difficult to review systematically in full. The study demonstrated that AI can audit these documents to surface quality and safety gaps that might otherwise persist undetected for years, not by making clinical decisions, but by solving the unstructured text problem and turning heterogeneous documentation into structured, reviewable data.
Obolenski described the framework as conceptually close to real-world implementation, noting that it was developed and tested within an operational clinical quality-management environment. The main barriers to broader adoption, he said, are not primarily technical.
"Clinical SOPs are often fragmented across heterogeneous local documentation systems and maintained as unstructured free-text documents," he said. "In addition, institutions require clear governance structures regarding validation responsibilities, version control, traceability, accountability, and regulatory compliance."
He framed the core governance question directly: "Who ultimately carries responsibility if errors occur within safety-critical clinical processes? This is precisely why process-oriented AI in quality management should operate within a Human-in-the-Loop framework, where clinical experts remain responsible for contextual interpretation, final validation, and regulatory oversight."
Are existing harmonization frameworks enough?
On whether programs such as EARL accreditation are sufficient, Obolenski was measured. "EARL has played a central role in improving quantitative comparability and reproducibility across scanners and institutions, which is essential for PET as a quantitative imaging biomarker," he said. "At the same time, our findings suggest that technical harmonization alone may not fully capture the complexity of routine clinical workflows. Many clinically relevant variations arise not at the scanner calibration level, but within operational processes."
He described AI-supported quality management as complementary to rather than replacing existing frameworks.
"The next step in harmonization may need to become more process-oriented and continuous," he said. "AI-supported quality-management approaches should be viewed as an additional layer supporting transparency, traceability, and continuous process alignment within increasingly complex imaging environments."
The authors note that the study is a single-center proof of concept and that scalability across institutions requires prospective multicenter validation.
The full paper is open access and available here.