Which image postprocessing techniques are best for evaluating tumors of the trachea and bronchus? Multiplanar reformations, volume rendering, and virtual bronchoscopy each have their roles, concludes a new study in PLOS One.
Researchers from China and the U.S. used MDCT to examine 31 patients with primary trachea and bronchus tumors, processing images with multiplanar reformatting, volume rendering, and virtual bronchoscopy techniques. They assessed each technique's ability to determine tumor location, morphology, extramural invasion, and extent of luminal stenosis, among other factors.
They concluded that no visualization technique was 100% effective at analyzing tumors. The results were consistent with those of surgery and pathology, with specific techniques working better in certain situations (PLOS One, September 2, 2015).
In fact, each technique has advantages and disadvantages, and all three may work best together, wrote lead author Mingyue Luo from Sun Yat-sen University in Guangzhou, China, along with colleagues from Tsinghua University in Shenzhen and Massachusetts General Hospital in Boston.
Variety of approaches needed
Tumors of the primary trachea and main bronchus have very different features owing to different growth modes and development directions, according to the authors. Tumor types include the following:
- Endoluminal nodular tumors with narrow bases: These nodular masses protrude into the endolumen with narrow bases or peduncles connected to walls, no thickened walls, and homogenous densities.
- Endoluminal nodular tumors with wide bases: These nodular masses protrude into the endolumen with wide bases, locally thickened walls, and homogeneous densities.
- Intraluminal and extraluminal tumors: These manifest as infiltrated growth along thickened walls, with invasion extraluminally, and masses both intraluminally and extraluminally.
Tumors with dominant intraluminal growth have significant luminal stenoses, the group noted. Tumors with evident extraluminal growth may resemble mediastinum tumors. Tumors with apparent intraluminal and extraluminal growth have large masses and are often obstructive.
While CT is a workhorse modality with many applications, the use of advanced imaging reconstruction can facilitate the assessment of tracheal and main bronchus tumors by overcoming the limitations of the traditional axial imaging plane, providing more anatomically and diagnostically useful information, the authors wrote. The study aimed to determine which image processing techniques are optimal for tumor detection and evaluation.
"Though CT is the most important noninvasive method for detection of primary trachea and main bronchus tumors, ordinary CT and ordinary spiral CT cannot disclose the entire structure of the trachea and main bronchi, and their detection is not accurate," they wrote.
MDCT of bronchus and trachea
All images for the study were acquired on a LightSpeed QX/i CT scanner (GE Healthcare) set at 2.5-mm collimation and 3.0 pitch. All patients had a precontrast CT scan of the chest from the thoracic inlet to the base of the lung, followed by scanning with contrast.
The image data were reconstructed using 1.5-mm sections and 0.5-mm intervals, and postprocessing was performed on a workstation using commercially available software (Advantage Workstation 4.5, GE Healthcare). Axial, coronal, sagittal, and oblique multiplanar reconstruction (MPR) images were acquired section by section, centering on trachea and main bronchus tumors to show the walls, lumina, and adjacent structures, the group wrote.
Overall, detection results with MDCT and multiplanar reformatting, volume rendering, and virtual bronchoscopy were consistent with surgery and pathology results, showing the following:
- Tumor locations (19 tracheal, 6 right main bronchi, and 6 left main bronchi)
- Tumor morphologies (2 endoluminal nodes with narrow bases, 13 endoluminal nodes with wide bases, and 16 both intramural and extramural masses)
- Extramural invasions of tumors
- Longitudinal involvement of tumors
- Morphologies of luminal stenoses (26 irregular, 3 circular, 1 eccentric, and 1 conical)
- Extent of tumors (5 mild, 7 moderate, and 19 severe)
Comparing the techniques
Each advanced reconstruction technique has unique advantages. MPR was used to obtain 2D multiplanar images centering on the trachea; it can reflect different tissue densities by using different attenuation scales with high-density resolution and no obvious artifacts, Luo and colleagues wrote.
The results demonstrated that MPR could not only display the locations, morphologies, internal features, and extramural invasions of primary trachea and main bronchus tumors, along with morphologies and extents of luminal stenoses, it could also measure their longitudinal involvement and distances between main bronchus tumors and trachea carinae. However, due to the 2D images, MPR could not provide a 3D effect, according to the researchers.
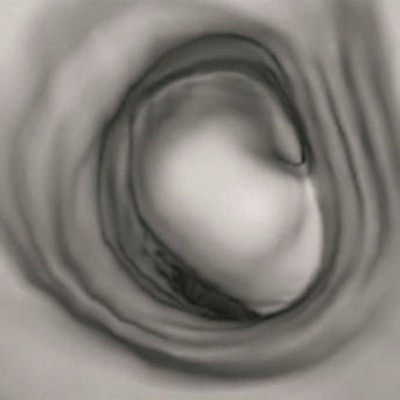
 Adenoma in trachea carina. MDCT axial (A), MPR (oblique, B), and virtual bronchoscopy (C) images. The images revealed a mass that protruded into the endolumen with a narrow peduncle connected to wall, no thickened wall, severe eccentric luminal stenosis, and homogeneous density without obvious enhancement. Images republished with permission of PLOS One, September 2, 2015.
Adenoma in trachea carina. MDCT axial (A), MPR (oblique, B), and virtual bronchoscopy (C) images. The images revealed a mass that protruded into the endolumen with a narrow peduncle connected to wall, no thickened wall, severe eccentric luminal stenosis, and homogeneous density without obvious enhancement. Images republished with permission of PLOS One, September 2, 2015.

Regarding volume rendering, the group noted that it is an improvement over other postprocessing techniques such as shaded surface display, maximum-intensity projection, minimum-intensity projection, and tissue transition projection, which carry the disadvantage of losing large amounts of data in the final reconstruction.
Overall, volume rendering produces well-differentiated displays with good contrast resolution and differentiation of tissues, the authors wrote. It maintains spatial relationships from initial data with less loss of imaging information and also true 3D effects, and it allows the local magnification and rotation of images to examine tumors closely.
Volume-rendered images can handily demonstrate locations, morphologies of primary trachea and main bronchus tumors, and morphologies and extents of luminal stenoses, and it can measure the longitudinal involvements and distances between main bronchus tumors and trachea carinae. However, volume rendering can't display the internal features of tumors and extramural invasions, they noted.
Finally, virtual bronchoscopy enables 3D visualization of the lumen and wall of the trachea and main bronchus in a manner similar to that of conventional optical bronchoscopy, and it can display tumors similarly to virtual colonoscopy, showing surface morphologies and proximal regions, Luo and colleagues wrote.
They found that virtual bronchoscopy could competently display morphologies, longitudinal involvements of primary trachea and main bronchus tumors, and morphologies and extents of luminal stenosis. However, virtual bronchoscopy cannot display accurate locations, internal features, extramural invasions, or distances between the main bronchus tumors and trachea carinae.
"MDCT and its MPR, volume rendering, and virtual bronchoscopy images have respective advantages and disadvantages," the group concluded. "Their combination could complement each other to accurately detect locations, natures, and quantities of primary trachea and main bronchus tumors with crucial information for surgical treatment."



















