MANCHESTER - Analysis of radiology reports generated using voice recognition software has shown an unacceptably high error rate, and urgent measures are essential to combat the problem, delegates learned at this week's U.K. Radiological Congress (UKRC 2017).
 UKRC 2017 and the U.K. Radiation Oncology Congress took place at the Manchester Central exhibition complex from 12 to 14 June.
UKRC 2017 and the U.K. Radiation Oncology Congress took place at the Manchester Central exhibition complex from 12 to 14 June.Voice recognition technology has been available for over three decades, and increasing numbers of radiologists are using it. Studies have shown that use of the software significantly reduces report turnaround time, explained Dr. Abul Haque, from the department of radiology at Queen's Hospital, in Burton-upon-Trent, U.K.
"The removal of a transcriptionist means a reduction in the cost per report and therefore a decrease in overall expenditure to the radiology department," he noted. "Quicker and less expensive reporting leads to increased workflow and therefore means a more productive and cost-effective radiology department overall."
Haque and his colleagues looked at the error rate of voice recognition reports generated by the seven qualified radiologists at the Queen's Hospital. They completed their retrospective audit in November 2016, and it made use of the 2016 guidelines from the Royal College of Radiologists (RCR) on voice recognition system report accuracy. The guidelines state that errors can be classified into the following three categories:
- Minor -- e.g., use of "am" instead of "an"
- Moderate -- incorrect words/syntax are used, making interpretation more difficult
- Major -- when the report makes no sense
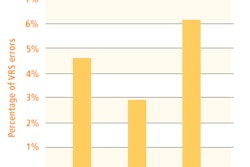
The overall error rate should be less than 5%, and major errors should be zero, according to the RCR.
The Queen's Hospital team used the clinical record information system to identify verified reports generated between 1 January and 30 April 2016. For each radiologist, they studied reports from four different modalities: plain film, ultrasound, CT, and MRI. For each modality, they randomly selected three reports per month, making a total of 12 reports per modality over the four months. They analyzed 48 reports overall per consultant and studied 336 reports for the seven radiologists.
Only 294 reports (87.5%) contained no errors. The remaining 42 reports (12.5%) had at least one error. Of these 42 reports, 36 (86%) were minor, five (12%) were moderate, and one (2%) was major.
The overall error rate of the hospitals in the vicinity is 12%, which is 7% more than the RCR recommendation, Haque pointed out. The overall major error rate of 0.3% for the hospital group is also above the RCR guidance of 0%.
To improve the situation, the following measures have been introduced at Queen's:
- Proofread all reports at least once before authorizing.
- If interruptions occur during a report, then switch off the dictating machine immediately and resume after interruption has been resolved.
- Consider macros (templates) for an unremarkable/normal scan because this will lessen the use of voice recognition and therefore reduce the risk of potential errors.
The results of the audit were presented in December 2016 at the radiology departmental audit meeting of the National Health Service trust (or hospital group). The plan now is to carry out another audit in summer 2017 and present the findings at a subsequent departmental meeting.
Haque's co-authors in this study were Drs. Moustafa El-Badawy and Sardar Qasim.