Susceptibility-weighted imaging (SWI) has emerged as an extremely useful tool for the diagnosis of different brain pathologies, and it is essential for radiologists to understand the principles and the clinical applications, according to Australian researchers.
“SWI is a 3D T2* weighted gradient echo sequence that takes advantage of phase and magnitude to enhance the visualisation of cerebral paramagnetic and diamagnetic substances,” explained Dr. India Plath and Prof. Alan Coulthard, from the Department of Medical Imaging, Royal Brisbane and Women’s Hospital. “It was initially designed to assess deoxyhemoglobin in veins and cerebral microbleeds, however its clinical applications have significantly widened and it is becoming increasingly useful in the diagnosis of a variety of neurological conditions.”
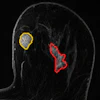
 (A) MRI brain SWI axial scan shows left frontal lobe lesion with mass effect and blooming artefact representing microhemorrhages within the lesion (note that contrast was given to the patient prior to acquisition of SWI images). (B) MRI brain SWI phase images axial: haemorrhagic lesion shows a bright/positive shift on the phase image due to paramagnetic susceptibility effect. All figures courtesy of Dr. India Plath and Prof. Alan Coulthard, Department of Medical Imaging, Royal Brisbane and Women’s Hospital.
(A) MRI brain SWI axial scan shows left frontal lobe lesion with mass effect and blooming artefact representing microhemorrhages within the lesion (note that contrast was given to the patient prior to acquisition of SWI images). (B) MRI brain SWI phase images axial: haemorrhagic lesion shows a bright/positive shift on the phase image due to paramagnetic susceptibility effect. All figures courtesy of Dr. India Plath and Prof. Alan Coulthard, Department of Medical Imaging, Royal Brisbane and Women’s Hospital.
SWI is particularly sensitive to venous blood, hemorrhage, and iron storage. Its main applications in clinical practice include trauma, vascular malformations, arterial ischemia, neurological tumors, and neurodegenerative diseases, they continued.
In trauma imaging, diffuse axonal injury (DAI) is a type of brain injury where torsional forces generated by rapid acceleration or deceleration of the head can result in shearing of axons and small punctate hemorrhages within the deep subcortical white matter. Areas most vulnerable to shearing include the cerebral gray-white matter junction, brain stem, splenium, and basal ganglia, and the extent of axonal injury and brainstem involvement tends to correlate with poor prognosis.
“Noncontrast CT of the brain is routine in patients with head injuries. Unfortunately, it is not sensitive to identify subtle DAI, and patients with relatively normal CT images may have significant neurological deficits,” the researchers stated. “Studies have demonstrated SWI is more sensitive than CT or other gradient echo flip sequences at detecting DAI and assessing the volume and distribution of lesions.”
Arteriovenous malformations (AVMs) usually present at birth and can grow with age, and they are characterized by high-flow and can generally be detected by conventional MRI techniques. In contrast, low-flow vascular malformations, including cerebral cavernous malformations (CCMs), may not be well defined on fast spin-echo sequences, and SWI provides increased sensitivity for low-flow vascular malformations.
 MRI brain axial SWI shows a well-defined lesion in the left posterior frontal/anterior parietal lobe. Prominent susceptibility artefact on SWI due to paramagnetic effect from hemosiderin deposits. The lesion had a lobulated appearance on T1 and T2 with no surrounding edema and was confirmed as a cerebral cavernous malformation.
MRI brain axial SWI shows a well-defined lesion in the left posterior frontal/anterior parietal lobe. Prominent susceptibility artefact on SWI due to paramagnetic effect from hemosiderin deposits. The lesion had a lobulated appearance on T1 and T2 with no surrounding edema and was confirmed as a cerebral cavernous malformation.
CCMs are composed of abnormally large capillary cavities surrounded by a single layer of endothelium. MRI findings are variable, depending on the presence of calcification and haemorrhage within the lesion. Recurrent microhemorrhages can occur within the lesion and may contain deoxyhemoglobin acutely or hemosiderin chronically, both of which will appear dark on SWI, they added.
An acute cerebral infarct occurs due to thromboembolism or atherosclerotic stenosis of a vessel. Vascular occlusion, through reduction in arterial blood flow, contributes to increased pooling of deoxygenated blood and high concentration of deoxyhemoglobin. SWI can provide information about the presence of hemorrhage within the infarction area, enabling differentiation of hemorrhagic transformation in ischemic stroke, according to Plath and Coulthard.
 A 68-year-old woman with delayed presentation of right middle cerebral artery occlusion with hemorrhagic transformation. MRI brain SWI axial scan shows multiple hypointensities in the right frontotemporal region in keeping with hemorrhagic transformation.
A 68-year-old woman with delayed presentation of right middle cerebral artery occlusion with hemorrhagic transformation. MRI brain SWI axial scan shows multiple hypointensities in the right frontotemporal region in keeping with hemorrhagic transformation.
“SWI can assist in the grading of cerebral tumors as it provides identification of both hemorrhagic and calcified foci within tumors and enables assessment of internal angioarchitecture,” they pointed out in research presented at the annual scientific meeting (ASM) of the Royal Australian and New Zealand College of Radiologists (RANZCR). “Calcification is diamagnetic and hemorrhage is paramagnetic, therefore resulting in opposite signal intensities on SWI phase imaging.”
In multiple sclerosis (MS), recent updates to the McDonald Criteria in 2024 include two new imaging markers -- central vein sign (CVS) and paramagnetic rim lesions (PRLs) -- to assist with the diagnosis of multiple sclerosis. These imaging markers can be seen on SWI. The CVS is due to the perivenular distribution of the demyelinating lesions around small cerebral veins. PRLs are specific for MS and represent chronic inflammation with iron accumulation in microglia at the lateral edge of chronic demyelination lesions, which appears as a hypointense rim on SWI.
In patients with Parkinson’s disease (PD), neurons are damaged early in the progression of the disease. Nigrosome-1 is the largest nigrosome and contains a substantial amount of dopaminergic cells affected in PD. SWI can assist in the diagnosis of PD by the identification of the loss of the tail of nigrosome 1, otherwise known as the swallow-tail sign.
 (A) MRI brain SWI axial scan shows normal appearance of nigrosome-1, high signal in a linear shape within the substantia nigra. Also known as swallow tail sign. (B) MRI brain SWI axial: substantia nigra signal intensity reduced bilaterally, with loss of the hyperintense signal in nigrosome-1 in keeping with loss of swallow tail sign, which may reflect Parkinson’s disease.
(A) MRI brain SWI axial scan shows normal appearance of nigrosome-1, high signal in a linear shape within the substantia nigra. Also known as swallow tail sign. (B) MRI brain SWI axial: substantia nigra signal intensity reduced bilaterally, with loss of the hyperintense signal in nigrosome-1 in keeping with loss of swallow tail sign, which may reflect Parkinson’s disease.
How SWI works
Magnetic susceptibility is a physical characteristic that defines how a substance responds when exposed to an external magnetic field. Diamagnetic substances, such as lipids, water, calcium, and myelin, have all their electrons paired and are repelled by the magnetic field. In contrast, paramagnetic substances, such as iron or copper, have unpaired electrons, which results in positive magnetic susceptibility. Paramagnetic and diamagnetic substances alter the phase of local tissue, resulting in a change of signal, which SWI takes advantage of, Plath and Coulthard noted.
“SWI sequences are typically acquired in 3D to allow for thinner slices and smaller voxel size with flow compensation in all three directions to reduce artefact,” they wrote. “A key feature of SWI is that magnitude and phase information are used to construct a new source of contrast, enabling delineation of brain anatomy at a fine detail and enhances evaluation of different brain pathologies. To create SWI, the raw phase image undergoes several processing steps.”
SWI generates filtered phase images in which calcifications and blood products exhibit signal intensities inverse of each other. “It is important to note that the appearance of these products on SWI phase images depends on the handedness of the scanner,” they stated, adding that Siemens Healthineers and Canon Medical Systems employ left-handed references, causing blood products to appear bright, whereas GE Healthcare and Philips use right-handed references in which blood products appear dark.
You can read the full e-poster on the RANZCR 2025 website.