A team of Italian researchers has said lung ultrasound scans may be better than chest radiography for children with COVID-19. The recommendation comes from the findings of a small, observational study published on 21 April in Pediatrics.
The study included eight children and adolescents under the age of 18 with the novel coronavirus who were admitted to a hospital in Turin, Italy. The researchers found good alignment between lung ultrasound scans and chest x-rays, but ultrasound has the additional benefit of not exposing children to radiation, they noted.
"While the number of patients analyzed is small, the high concordance between radiologic and [lung ultrasound] findings suggests that ultrasound may be a reasonable method to detect lung abnormalities in children with COVID-19," wrote the authors, led by Dr. Marco Denina, a pediatric infectious diseases specialist from the Regina Margherita Children Hospital.
Lung ultrasonography has already proved useful for doctors needing to make diagnosis, treatment, and admission decisions for adult patients with COVID-19, but limited research has been conducted into its effectiveness for children with the novel coronavirus.
Researchers from Regina Margherita Children Hospital believed the benefits of point-of-care ultrasound (POCUS) would make it a good imaging candidate for children with COVID-19. They tested the modality's effectiveness with eight children admitted to the pediatric infectious diseases department between March 18 and March 26.
The severity of COVID-19 varied in the children. Two children had severe clinician symptoms that required noninvasive oxygen administration for two to four days. Another two had moderate symptoms, and four had mild symptoms. None of the children needed mechanical ventilation.
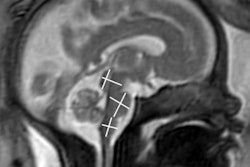
The majority of the children (5/7) showed confluent B-lines on their lung ultrasound scans, a similar finding to adults with COVID-19. Two of the children also showed subpleural consolidations on ultrasound scans. Like with adult patients, the children's lung ultrasound findings appeared to improve about a day before clinical symptoms got better.
In seven patients, the lung ultrasound findings aligned with the radiologic findings. The one patient whose findings did not match had a normal chest x-ray but interstitial B-lines on their lung ultrasound scan.
The findings demonstrate that lung ultrasound may be a valuable imaging modality for children with COVID-19, the authors noted. Lung ultrasound also has additional benefits over chest x-ray, including limiting the amount of radiation exposure for children, being able to be administered at patients' bedsides to limit their movement, and being easier to clean and disinfect when wireless, point-of-care ultrasound systems are used.
"Although further studies are needed to better understand and characterize [lung ultrasound] findings in this novel disease in children, we propose [lung ultrasound] routinely protocol examinations as a useful tool in the diagnostic and clinical management of mild/severe COVID-19 in children," they concluded.
Editor's Note: the photo used to introduce this article on the homepage is of Dr. Herma Holscher, a pediatric radiologist at Haga Teaching Hospital / Juliana Children's Hospital in The Hague, the Netherlands.