Adding 3-tesla MRI to mammography for patients presenting with suspicious microcalcifications adds "significant" value, Dutch researchers have found. Specifically, the modality boosts the percentage of ductal carcinoma in situ (DCIS) lesions detected.
Microcalcifications are common on mammography and constitute up to 31% of lesions detected at screening mammography, according to previously published research. DCIS often presents with microcalcifications on mammography -- up to 79% of mammographically detected DCIS lesions manifest with microcalcifications only -- so careful evaluation of these microcalcifications is essential (European Radiology, 29 September 2013).
"The benefit of MRI in a selected patient population with mammographically suspicious microcalcifications remains unclear," wrote Dr. Bertine Stehouwer, from the department of radiology at the University Medical Center Utrecht in the Netherlands, and colleagues.
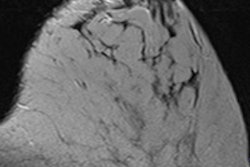
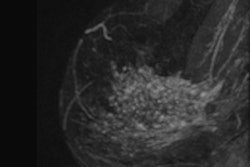
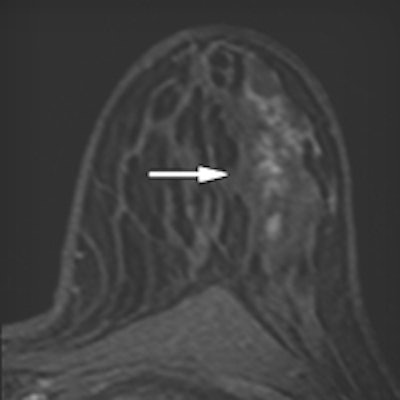
 Mammography and breast MRI results of a patient presenting with suspicious microcalcifications on mammography, classified as BI-RADS 4. Mammography (a, left mediolateral view) shows a cluster of microcalcifications which is shown enlarged in the inset. At breast MRI, both observers identified non-mass-like enhancement with a segmental distribution and clumped internal enhancement (b, arrow). Kinetic curve assessment showed a type I curve. The lesion was scored BI-RADS-MRI 4 and BI-RADS-MRI 5, respectively. Histopathology showed DCIS grade 3. All images reproduced from: B.L. Stehouwer, L.G. Merckel, H.M. Verkooijen, et al. 2013. 3-T breast magnetic resonance imaging in patients with suspicious microcalcifications on mammography. Eur Radiol. DOI 10.1007/s00330-013-3029-1.
Mammography and breast MRI results of a patient presenting with suspicious microcalcifications on mammography, classified as BI-RADS 4. Mammography (a, left mediolateral view) shows a cluster of microcalcifications which is shown enlarged in the inset. At breast MRI, both observers identified non-mass-like enhancement with a segmental distribution and clumped internal enhancement (b, arrow). Kinetic curve assessment showed a type I curve. The lesion was scored BI-RADS-MRI 4 and BI-RADS-MRI 5, respectively. Histopathology showed DCIS grade 3. All images reproduced from: B.L. Stehouwer, L.G. Merckel, H.M. Verkooijen, et al. 2013. 3-T breast magnetic resonance imaging in patients with suspicious microcalcifications on mammography. Eur Radiol. DOI 10.1007/s00330-013-3029-1.Previous studies using 1.5-tesla MRI in patients with microcalcifications report sensitivities between 45% and 87%, and specificities between 68% and 100%. Currently, European guidelines state in the case of mammographic microcalcifications, MRI is unable to exclude breast cancer so the decision to perform biopsy should be based on mammographic findings.
However, the use of 3-tesla MRI in patients with suspicious microcalcifications has not been investigated -- until now.
Stehouwer and team included 123 patients from the MR Mammography of Nonpalpable Breast Tumors (MONET) trial in their study. Between January 2006 and May 2009, patients with mammographically detected BI-RADS 3-5 microcalcifications underwent 3-tesla breast MRI (Achieva, Philips Healthcare) before breast biopsy. Two breast radiologists reviewed all MRI exams of the histopathologically confirmed index lesions.
The detection rate of invasive carcinoma and DCIS was evaluated, as well as the added diagnostic value of MRI over mammography and breast ultrasound.
At pathology, 40 of 123 (33%) lesions proved malignant, and 70% of those were DCIS, the rest were invasive carcinoma. The two observers detected all invasive malignancies at MRI, as well as 79% (observer 1) and 86% (observer 2) of in situ lesions. MRI in addition to conventional imaging led to a significant increase in area under the receiver operating characteristic (ROC) curve from 0.67 to 0.79 for observer 1 and to 0.80 for observer 2.
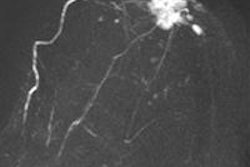
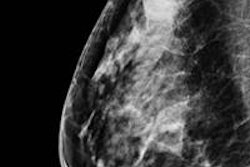
 Mammography and breast MRI results of a patient presenting with suspicious microcalcifications on mammography, classified as BI-RADS 4. Mammography (a, left exaggerated lateral craniocaudal view) shows a cluster of microcalcifications which is shown enlarged in the inset. At breast MRI, observer one identified nonmass-like enhancement with a regional distribution, heterogenous internal enhancement (b, arrow), and a type II kinetic curve. Observer two identified a non-mass-like enhancement as well, with a focal distribution, heterogeneous internal enhancement, and a type III kinetic curve. The lesion was scored BI-RADS-MRI 3 and BI-RADS-MRI 4, respectively. Histopathology showed an invasive lobular carcinoma and DCIS grade 1.
Mammography and breast MRI results of a patient presenting with suspicious microcalcifications on mammography, classified as BI-RADS 4. Mammography (a, left exaggerated lateral craniocaudal view) shows a cluster of microcalcifications which is shown enlarged in the inset. At breast MRI, observer one identified nonmass-like enhancement with a regional distribution, heterogenous internal enhancement (b, arrow), and a type II kinetic curve. Observer two identified a non-mass-like enhancement as well, with a focal distribution, heterogeneous internal enhancement, and a type III kinetic curve. The lesion was scored BI-RADS-MRI 3 and BI-RADS-MRI 4, respectively. Histopathology showed an invasive lobular carcinoma and DCIS grade 1."These results are concordant with previous research at 1.5T, using the same specific patient population, and therefore do not show improvement by moving to the higher field strength of 3T," the authors wrote. "Moreover, the difference between the readers shows that it is possible to read breast MRI at a higher sensitivity at the expense of specificity and vice versa. This implies that a reader must be aware of the a priori likelihood of malignancy when evaluating a breast MRI because this may influence the evaluation."
However, only low- and intermediate-grade DCIS are affected in this instance and not high-grade DCIS or invasive carcinomas -- in fact, almost all the DCIS lesions detected on MRI were high-grade in the study.
One of the limitations of the study is that too few cases were included to statistically evaluate the association of individual BI-RADS-MRI descriptors with the presence of malignancy. The same accounts for the multivariate analysis in which only imaging determinates were included, they wrote.
"Conventional imaging and MRI were used, whereas age and BMI [body mass]index] also showed significant difference in the univariate analysis," they added. "Unfortunately, the limited number of cases did not statistically allow for inclusion of more determinants."
Also, the researchers only included patients with microcalcifications seen on mammography. Thus, noncalcified DCIS lesions were not evaluated, although they also may show enhancement on MRI.
Lastly, the pathological size of the index lesions was not taken into account in the analyses.
"Obviously, a small lesion found at histopathology will be more difficult to detect and evaluate on MR imaging," the researchers note. "Also, the ability of 3T MRI to assess lesion extent, compared to histopathology, could not be evaluated. Lastly, no information was available on the reasons why breast ultrasound was performed or not."
Breast ultrasound helps evaluate if there is an associated mass that may indicate invasive disease.
"In the end, DCIS is regarded as a potential precursor lesion of invasive disease, and is therefore treated with breast-conserving therapy followed by radiation therapy," they wrote. "Our results do show an added diagnostic value of 3T breast MRI to conventional imaging, but unfortunately MRI does not exclude DCIS lesions of all grades sufficiently in all cases, and its sensitivity is not high enough to replace biopsy."
New MR techniques may evolve to visualize microcalcifications on breast MRI, and when ready for clinical use, one of these techniques might improve DCIS detection, the researchers concluded.