A study published online February 1 in the European Journal of Radiology found that dual-energy (DE) coronary CT angiography (CTA) outperformed SPECT for assessing myocardial perfusion in patients with suspected coronary artery disease.
The South Carolina researchers, who built a decision model comparing CT to SPECT and MRI, found that dual-source coronary CTA was the best deal by several measures.
"In a limited cohort of high-risk patients, dual-energy CT outperformed SPECT for the assessment of myocardial perfusion, with positive effects on cost-effectiveness in our model," study co-investigator U. Joseph Schoepf, MD, told AuntMinnie.com.
Long-term costs and outcomes
The study is among the first to assess the long-term costs and outcomes of coronary CTA versus the more commonly used SPECT exam, wrote Mathias Meyer, MD, Schoepf, and colleagues from the Medical University of South Carolina in Charleston, along with researchers from Mannheim-Heidelberg University in Germany and Catholic University of the Sacred Heart in Rome.
"While cardiac magnetic resonance imaging has demonstrated superiority in detecting physiologically significant perfusion defects due to coronary artery stenosis, single photon emission computed tomography is still the most widely used test for this purpose," Meyer and colleagues wrote (European Journal of Radiology, February 1, 2011).
However, the specificity of SPECT is limited, resulting in a relatively high false-positive rate when the pretest probability of disease is low, leading to unnecessary referrals for diagnostic catheter angiography, they wrote.
While anatomical testing, such as invasive coronary angiography, can directly visualize and grade coronary artery stenosis, it has limitations for grading the hemodynamic effect of lesions on myocardial perfusion, the authors explained. For that reason, a single test for the comprehensive evaluation of both stenosis and its effects on the heart would be ideal.
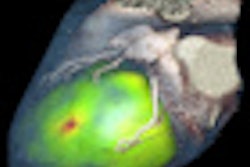
Dual-energy coronary CTA offers good diagnostic accuracy for detecting physiologically significant stenoses thanks to its ability to differentiate materials and quantify myocardial iodine distribution. Thus, DECT may be an effective standalone test for the comprehensive assessment of cardiac anatomy and morphology, function, perfusion, and viability.
"Until now no comparative data is available on the effectiveness of SPECT versus DECT for myocardial perfusion assessment in terms of lifetime benefits and healthcare expenditures," Meyer and his team wrote. "The purpose of this study was to compare diagnostic accuracy, incremental cost-effectiveness and gain in quality-adjusted life-years (QALYs) of SPECT versus DECT imaging for myocardial perfusion in workup of patients with [coronary artery disease (CAD)]."
The researchers developed a decision and simulation model to estimate the cost and health effects of using DECT myocardial perfusion imaging instead of SPECT for identifying patients who need catheter angiography and possible revascularization.
The study model was based on the performance indices of stress/rest DECT compared with stress/rest SPECT for detecting myocardial perfusion deficits in 50 patients (74% male; mean age, 61 ± 10 years; average body weight, 83 ± 21 kg) with coronary artery disease.
Nearly half of the patients (24/50) had a history of myocardial infarction, while 16 had no history of heart disease. Within two months after imaging, 10 of 50 patients underwent coronary artery bypass grafting due to severe two- or three-vessel disease, Meyer and colleagues wrote.
All patients had adenosine stress/rest perfusion scans and delayed enhancement cardiac MRI on a 1.5-tesla scanner (Magnetom Avanto, Siemens Healthcare, Malvern, PA) including contrast perfusion during peak adenosine (140 g/kg/min) stress and at rest.
At cardiac MR, delayed-enhancement scans were acquired 15 minutes after the last contrast injection. Both the perfusion and delayed-enhancement phases used single-shot short-recovery fast imaging with steady-state precession (SR-true-FISP) and T1-weighted sequences, TI of 250 msec, and TR of two cardiac cycles. Two experienced readers looked for perfusion defects and delayed enhancement by consensus using a 17-segment American Heart Association model, the team wrote.
At CT, all patients were scanned with a 64-detector-row dual-source CT scanner (Somatom Definition Flash, Siemens) in dual-energy mode. Calcium scoring was followed by prospectively gated coronary CTA using 70 mL of contrast, followed by a 50-mL saline flush administered in a triphasic protocol at 0.6-mm sections, 120 kV tube current, and 320 mAs.
Dose reduction to 25% of the nominal tube current was applied between 30% and 90% of the RR for functional analysis. Images were reconstructed using 0.75-mm section thickness and 0.3-mm reconstruction increment at 40% or 70% RR, depending on the heart rate. Myocardial perfusion imaging was performed in the "shuttle" mode during peak adenosine stress.
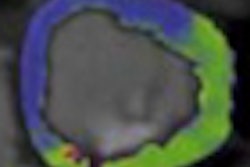
SPECT was performed after intravenous administration of technetium-99m using a one-day protocol. The Bruce treadmill protocol was used for ergometric stress testing, and a triple-head camera (Vertex 60+, Philips Healthcare, Andover, MA) with attenuation correction was used for electrocardiogram-gated data acquisition. Two observers working independently interpreted the studies for perfusion defects.
After imaging, all patients were classified as true-positive, false-positive, true-negative, or false-negative for perfusion defects using cardiac MRI results as the reference standard.
For DECT, the model assumed reimbursement of $1,700 per patient, but cardiac MRI costs were not included, while other healthcare costs were taken from the Medical University of South Carolina hospital billing system, the authors noted.
Results
Among the 50 patients 43 (86%) had perfusion defects at cardiac MRI, including 32 with fixed defects and 11 with reversible defects.
Cost, sensitivity, and specificity for DECT vs. SPECT
|
||||||||||||||||||
| ICER = incremental cost-effectiveness ratio. |
DECT was more sensitive than SPECT on a per-patient basis, the authors reported. Compared with cardiac MRI, dual-energy CT yielded 90% sensitivity, 71% specificity, and 87% accuracy for identifying patients with obstructive CAD. SPECT delivered 85% sensitivity, 57% specificity, and 79% accuracy compared with MRI.
The DECT strategy was far more cost-effective than SPECT. Compared with the no imaging and no treatment strategy, routine SPECT gained 13.49 QALYs with an incremental cost-effectiveness ratio (ICER) of $3,557 per QALY.
DECT's ICER was lower at $3,191 per QALY (p = 0.0002), garnering an additional 0.64 QALYs (total 14.13 QALYs) compared to the SPECT strategy.
Myocardial perfusion SPECT had a significantly higher average cost of $2,938 per patient (p = 0.0002), Meyer and colleagues wrote.
"Our study results indicate that cardiac DECT imaging has a high sensitivity (90%) and a good specificity (71%) for the qualitative assessment of myocardial perfusion," the group reported. These findings were in agreement with previous studies.
"Results for myocardial perfusion SPECT indicate a good sensitivity (85%) but only a poor specificity (57%) for qualitative assessment of myocardial perfusion, with a high rate of false-negative findings," they wrote.
The results of the cost-effectiveness analysis suggest that a strategy based on myocardial perfusion DECT for patients with known or suspected CAD "led to lower costs per patient and seems to be more effective than myocardial perfusion SPECT in prolonging life and ICER" when the diagnosis is correct, Meyer and colleagues wrote.
"Even when several parameters such as accuracy or myocardial perfusion defects prevalence were modified (between 10%-100% and 40%-80%, respectively), DECT remains cost-effective to SPECT in this study," they noted.
With CT, the authors used several radiation dose-lowering techniques to reduce dose to an average of 13 mSv, the equivalent of a one-day single-isotope technetium SPECT scan.
As for limitations, outcomes were sparse in the clinical subgroups, the team noted, and QALYs "might not be the best outcome criteria for evaluating cost-effectiveness of imaging tests," they wrote. Additional studies will be needed to assess CT's potential for the diagnostic imaging of all aspects of coronary heart disease.
"Using myocardial perfusion DECT as a first-line imaging test for the workup of patients with CAD might provide gains in QALYs while lowering costs if compared to routine myocardial perfusion SPECT," according to the authors.
Larger multicenter studies in a general patient population will be needed to validate the performance of dual-energy CT, and the cost-effectiveness of this approach will ultimately also depend on the prognostic value of DECT findings, which has not yet been assessed, and on the eventual cost of a dual-energy CT study, which has not been firmly established for clinical use, Schoepf told AuntMinnie.com.
"However, our preliminary results bode well for the potential prominent role of dual-energy CT in the noninvasive, comprehensive assessment of cardiac structure and function in the diagnostic workup of coronary heart disease," he said.
| Schoepf reported that he receives research support and is a consultant for Bayer HealthCare Pharmaceuticals, Bracco, GE Healthcare, Medrad, and Siemens. The other authors had no conflicts to disclose. |
By Eric Barnes
AuntMinnie.com staff writer
February 2, 2011
Related Reading
3D MRI stress perfusion accurate for myocardium evaluation, January 25, 2011
Dual-phase DECT myocardial perfusion cuts time, dose, January 4, 2011
Adenosine stress DECT equivalent to SPECT, MRI, November 21, 2008
Dual-source CT edges into cardiac SPECT turf, March 6, 2008
CTA predicts functional recovery of the myocardium, September 7, 2007
Copyright © 2011 AuntMinnie.com