PARIS - The new guidelines from the European Society of Cardiology (ESC) are unequivocal in strongly recommending functional testing before any invasive procedure for myocardial revascularization. Yet the choice of a test is left to the cardiologist, who faces an increasing number of techniques and conflicting evidence.
At the annual ESC congress, being held this week in Paris, the conundrum was elevated to the level of a controversy in a debate titled, "Cardiac magnetic resonance imaging has replaced nuclear."
 The ESC congress, Europe's largest medical meeting, attracts around 30,000 participants a year and is taking place in Paris from 27 to 31 August.
The ESC congress, Europe's largest medical meeting, attracts around 30,000 participants a year and is taking place in Paris from 27 to 31 August.
Passionately advocating for a shift from the widely used SPECT test to the emerging technique of cardiac MRI was Dr. Eike Nagel, a professor of clinical cardiovascular imaging at King's College London. Dr. Juhani Knuuti, from the PET Centre at Turku University Central Hospital in Finland, was equally spirited in his defense of nuclear testing.
Cardiologists should choose the optimal functional test, which is clearly cardiac MRI, Nagel stated. Its superiority over SPECT was demonstrated by the Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease (CE-MARC) trial, the results of which are now in press with the Lancet. Cardiac MRI provides quantitative data that move away from yes-no decisions for revascularization to decisions based on stenosis severity and informed by the extent of the stenosis, including its location and flow, he said.
Whereas SPECT provides a resolution of 10 x 10 mm, or a single volumetric pixel (voxel), the resolution of an MRI functional examination is 3 x 3 mm or 10 voxels.
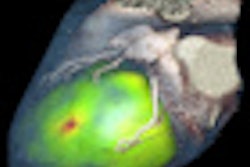
The need for higher spatial resolution is nicely explained, Nagel said, by looking at the physiology of stenosis in the endocardium, where ischemia begins. Greater resolution also enables a microvessel flow examination to not only indicate if there is ischemia but also show what kind of ischemia exists and its significance for the patient.
Finally, a key factor in the decision is radiation exposure of the patient.
"We should not reduce radiation by optimizing our techniques, but should try to move away from it altogether using a technology that gives the same answer without radiation," Nagel said.
Cardiac MRI examinations take too long, and the lack of MRI capacity at most centers helps to explain the lower adoption rate, countered Knuuti. Instead of debating the merits of the two modalities, he urged cardiologists to simply choose the most available technique, and there is an overwhelming body of evidence for SPECT across sensitivity, specificity, and reproducibility.
"I do not diagnose voxels. The clinical message is whether this is ischemia or not. The rest is technical jargon," he said. "For 20 years we have been hearing that MRI is going to replace SPECT in a couple years. But look at the numbers. There are 2,400 SPECT scans per million people in Europe and a fraction of this for cardiac MRI exams at less than 500 per million people."
Knuuti then challenged Nagel's claim for superiority by placing the recent cardiac MRI trial within the context of a meta-analysis of SPECT studies. The result makes Nagel's claim seem artificial, he said.
"MRI is great, if you have the experience with it," he said. "But the power of MRI is somewhere other than in cardiac disease."