Middle meningeal artery embolization for chronic subdural hematoma has moved from experimental to routine, but patient selection, embolic agent choice, and the role of surgery remain open, as a session at RöKo Digital 2026 made clear.
Chronic subdural hematoma is one of the most common conditions in neurosurgery, and one whose incidence is set to rise further. The reason is demographic: the patient group at highest risk, people of ages approximately 75 and above, will grow substantially over the coming decades.
With the demographic shift grows the need for treatment options suitable for older, multimorbid patients. Embolization of the middle meningeal artery has gained ground in this context as an increasingly established therapeutic option, a trend supported by current data from Germany, presented at the DRG Refresher Course on Neuroradiology.
From pathophysiology to intervention
Chronic subdural hematoma does not arise from a single bleeding event alone but from a self-perpetuating cycle. A border cell membrane forms at the dura, immature and fragile vessels grow into it, rupture, and cause repeated microbleeds.
Because these pathological vessels are supplied by the middle meningeal artery, embolization targets exactly this point, interrupting the blood supply to the membrane and enabling the body to resorb the hematoma.
Eight randomized controlled trials involving more than 2,700 patients are now available, comparing MMA embolization in addition to standard management against standard management alone, Dominik Vollherbst, an interventional radiologist at Heidelberg University Hospital, told the course.
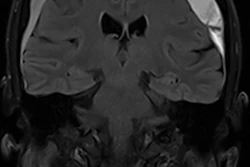
 Flat-detector CT showing catheter position following contralateral middle meningeal artery embolization in a case where ipsilateral access was not possible.Dominik Vollherbst, Heidelberg University Hospital/DRG Refresher Course on Neuroradiology, RöKo Digital 2026
Flat-detector CT showing catheter position following contralateral middle meningeal artery embolization in a case where ipsilateral access was not possible.Dominik Vollherbst, Heidelberg University Hospital/DRG Refresher Course on Neuroradiology, RöKo Digital 2026
Six of eight trials were positive, demonstrating a reduction in treatment failure and an overall low procedural complication rate. Applying these results to clinical practice, Vollherbst suggested, would mean that almost every patient presenting with chronic subdural hematoma should be considered for embolization, while acknowledging that routine clinical reality at most centers still looks different.
At Heidelberg, two patient groups are preferentially treated: those with recurrent hematoma following surgery, and those on anticoagulation therapy in whom surgical risk is elevated and interruption of therapy needs to be minimized.
German data from Düsseldorf
Keihan Darvishi from Düsseldorf University Hospital presented results of a retrospective single-center study on particle embolization using PVA particles of 150 to 250 μm. Of 36 patients with 42 embolizations, 90.5% with recurrent hematoma after initial surgery, 80% showed significant hematoma reduction, from a median of 17 mm to 7 mm.
Neurological improvement of at least one mRS point was documented in 78% of patients. The complication rate was 9.5%, exclusively minor, no patient sustained permanent neurological deficit.
The 20% treatment failure rate requires closer reading: 87.5% of these cases had a follow-up of under ten days, representing very early recurrence not necessarily attributable to the embolisation itself. Darvishi estimates the true embolization-associated recurrence rate at approximately 4%.
Technical practice and other open questions
The subsequent discussion at the course revealed that the choice of embolic agent, liquid embolisates such as Onyx or PHIL versus PVA particles, varies between German-speaking centres.
Vollherbst favors liquid embolisates, partly because most of the positive randomized trials were conducted with these agents. Darvishi and the Düsseldorf team use PVA particles and regard them as an effective, safe, and cost-efficient option, even though the procedure takes longer than with liquid embolisates.
There was common ground that the relevant anastomoses to the orbit, skull base, and petrous bone must be identified, and that maintaining a safety distance of approximately one cm from these areas substantially reduces the complication risk. Vollherbst recommends flat-detector CT after embolization as a routine step to verify embolic agent distribution.
The central open question remains patient selection: who benefits from embolization alone, who from the combination with surgery, and who still requires classical surgical drainage?