Individuals who are known to use cocaine and who present with a suspected overdose should also be thoroughly investigated -- including with imaging -- to exclude other causes of their presentation such as infection, according to a group of authors from Malta.
In an article published online by BMJ Case Reports, Dr. Kelly Gatt and colleagues from the department of infectious diseases at Mater Dei Hospital in Msida shared a case involving a 38-year-old man known to be a heavy cocaine user.
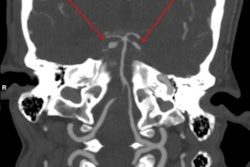
After initially presenting with right orbital swelling, an examination of his fauces showed erosion of the hard and soft palate. A subsequent CT scan confirmed palatal destruction. The patient had no signs of orbital cellulitis so the clinicians diagnosed preseptal cellulitis. He was then placed on intravenous antibiotics and his condition improved enough after seven days to be discharged, according to the authors.
However, the patient returned four months later with a suspected overdose, obtunded with a Glasgow coma scale (GCS) score of 9. He was started on 4.5 g of piperacillin/azobactam empirically and was resuscitated with intravenous fluids. A neurological exam then revealed a new right hemiplegia, and an urgent head MRI scan showed new fluid collection and soft-tissue swelling at the craniocervical junction causing myelopathy.
The clinicians also observed pachymeningitis. Although the man's antibiotic was then switched to ceftriaxone and Metronidazole to enable better penetration of the blood-brain barrier, the patient unfortunately passed away shortly afterward.
"Intranasal cocaine users presenting without an obvious source of infection should have thorough examination of their palate and imaging of the head as required," noted Gatt and colleagues, adding that the case highlights the need for vigilance when drug users present with a suspected overdose.
"Other causes of deterioration in their general condition should be explored prior to attributing a low GCS to illicit drug use," they wrote. "In such cases, thorough history and examination is required. If available, collateral history should always be taken."