Female genitourinary malformations are not all that common; however, diagnostic imaging for these anomalies is important. Researchers from Spain detail what to look for in a new article published this month in Insights into Imaging.
Drs. Pedro Acién and Maribel Acién from Miguel Hernández University in San Juan discussed abnormalities such as uterine duplicity and hypoplasia of a urogenital ridge, explaining what to look for. These types of abnormalities can be associated with a range of gynecological and obstetric problems, they noted.
"Diagnostic imaging for all these anomalies is essential," the authors wrote (Insights Imaging, 9 August 2016).
Why malformations matter
While female reproductive abnormalities occur in only 3% to 6% of the population, it is important to identify them, as they're associated with a range of gynecological and obstetric problems, according to the authors, from the university's departments of public health and scientific health, as well as the department of gynecology.
Complex malformations, such as mesonephric and some Müllerian anomalies, cloacal or urogenital sinus anomalies, and malformative combinations are especially important, because they can create fertility problems, cause clinical symptoms, and impact quality of life, especially in young women, they added.
Imaging and cataloguing of female genital malformations are important, but they require knowledge of the female genitourinary tract that not all radiologists have, such as the embryology of the tract and interaction between the Wolffian/Müllerian ductal systems and also the anomalies involved in the classical Müllerian development and the septum resorption processes.
To help radiologists, the authors examined the clinical presentation, cataloging, and inclusion of female genital malformations in the embryological and clinical classification in other current classification systems in their research.
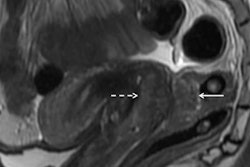
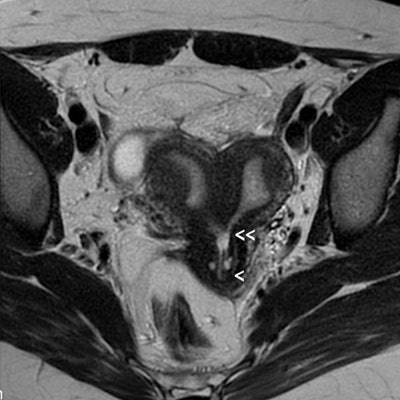
 A 32-year-old woman with complete unilateral vaginal or cervicovaginal agenesis or atresia and huge endometrioma. A: T2-weighted MR image shows a bicornuate (transitional or bicorporeal septate) uterus with communication at the isthmic level (
A 32-year-old woman with complete unilateral vaginal or cervicovaginal agenesis or atresia and huge endometrioma. A: T2-weighted MR image shows a bicornuate (transitional or bicorporeal septate) uterus with communication at the isthmic level (Examples of malformations
The main classification systems for female genital malformations refer to only Müllerian anomalies or the anatomic visual appearance, and they don't explain or suggest the origin of these malformations or their appropriate therapeutic correction, the authors wrote.
This makes the embryological classification a better choice, because it correlates with clinical presentations among vaginal anomaly, uterine anomaly, and ipsilateral renal agenesis or renal dysplasia with or without ectopic ureter. It also suggests the origin and possible clinical presentation. This leads to diagnostic imaging, they added.
For instance, in cases of agenesis or hypoplasia of a urogenital ridge, there will be the absence of the kidney, ureter, ovary, fallopian tube, hemiuterus, and hemivagina. Clinically, the most common presentation is a unicornuate uterus without a rudimentary horn or contralateral tube and ovary, the researchers found.
"This condition is sometimes associated with skeletal and/or auditory," they wrote. "If there is also contralateral Müllerian agenesis, the diagnosis will be Rokitansky syndrome with unilateral renal agenesis or atypical Rokitansky."
MRI is the best modality for imaging these malformations, complemented with hysterosalpingography if unicornuate uterus is present.
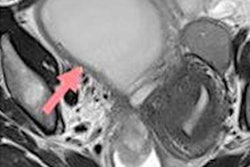
 Cases with vaginal or cervicovaginal atresia or agenesis and normal uterine corpus. A: T2-weighted MR image in a 20-year-old woman with complete cervicovaginal atresia. Medial sagittal section showing the uterus and cervicovaginal atresia (
Cases with vaginal or cervicovaginal atresia or agenesis and normal uterine corpus. A: T2-weighted MR image in a 20-year-old woman with complete cervicovaginal atresia. Medial sagittal section showing the uterus and cervicovaginal atresia ("It should be noted that renal agenesis occurs because of lesions of the urogenital ridge and not because of Müllerian agenesis," the authors wrote.
The combination of uterine duplicity and obstructed or blind hemivagina appears to be virtually always associated with ipsilateral renal agenesis or dysgenesis, and imaging tests are necessary to confirm the absence of a normal kidney on the affected side and also to detect abnormalities of the contralateral kidney and ureter, they added.
If there is unilateral renal agenesis, there must also be genital malformation with didelphys, bicornuate, and, more rarely, septate uterus (sometimes reported as single uterus), but not necessarily a blind or atretic hemivagina. There could also be cases with partial reabsorption of the vaginal septum, they continued.
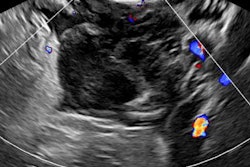
![Urogenital sinus anomalies. MR images [(1) T1- and (2) T2-weighted fat-suppressed images in the sagittal plane] show a retrovesical blind vagina with apparent inferior half atresia and undetected fistula tract to the bladder (](https://img.auntminnieeurope.com/files/base/smg/all/image/2016/08/ame.2016_08_26_16_04_51_413_female_genital_malformationspic3.png?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) Urogenital sinus anomalies. MR images [(1) T1- and (2) T2-weighted fat-suppressed images in the sagittal plane] show a retrovesical blind vagina with apparent inferior half atresia and undetected fistula tract to the bladder (
Urogenital sinus anomalies. MR images [(1) T1- and (2) T2-weighted fat-suppressed images in the sagittal plane] show a retrovesical blind vagina with apparent inferior half atresia and undetected fistula tract to the bladder (Differentiating between a bicornuate and a septate uterus also is controversial. The distinction is important for the treatment of symptomatic patients (abdominal Strassmann metroplasty on the bicornuate uterus versus hysteroscopic resection in cases of septate). Transvaginal ultrasound, 3D ultrasound, sonohysterography, and especially MRI have ushered in a new era of noninvasive diagnosis of uterine anomalies.
"Nevertheless, there are transitional cases between both uterine segments in which fusion defects are associated with resorption defects, and these situations must also be recognized before a therapeutic decision can be made," the authors added.
Another takeaway from their article is that the anomalies most frequently diagnosed incorrectly are the distal mesonephric anomalies, which are associated with unilateral renal agenesis or renal dysplasia with ectopic ureter.