HAMBURG - MRI can be used to detect endometriomas, difficult-to-detect cells from the lining of the uterus found outside the uterine cavity, and also guide surgical intervention, according to a presentation from the 95th congress of the German Society of Radiology (DRK), 28-31 May.
 Dr. Julia Wenzel conducted a study that demonstrates MRI supports detection of endometriomas.
Dr. Julia Wenzel conducted a study that demonstrates MRI supports detection of endometriomas.
Every tenth woman suffers from endometriosis, which can cause infertility and pain. Endometriomas are difficult to detect, but MRI can help, according to a study conducted by Dr. Julia Wenzel from the department of diagnostic and interventional radiology at Giessen University Hospital in Marburg, Germany.
Endometrial cells are influenced strongly by estrogen and progesterone levels, which lead to expansion in the days preceding ovulation, with perfusion increasing, and with increased amounts of exudate being produced. As the end of the menstrual cycle approaches, the influence of progesterone is reduced; this leads to the ejection of the lining of the uterine endometrium during menorrhea.
"While this is a normal process in the uterus, it produces problems in endometriomas located in other body regions," Wenzel said in her presentation. "Detecting these lesions presents a major challenge to surgeons. They can be very small, and in certain cases deeply infiltrating into tissue."
Endometriomas may be found in places such as on the ovaries, on the bowel wall, or on the bladder. Removal by surgical intervention is the standard treatment.
The challenge
Sonography does not provide a complete picture. Can MRI help? Wenzel conducted a study enrolling 131 patients, comparing preintervention MRI evaluations with reports from the operating room and pathology regarding the endometrial tissue removed surgically.
 Source: Dr. Julia Wenzel.
Source: Dr. Julia Wenzel."Endometriomas can take on a variety of phenotypes, including cysts and adhesions, which adds to the difficulty of identifying them in MR images," Wenzel said.
Nevertheless, in the study, the experts detected 81% of 392 tissue samples of varying sizes verified by pathologists.
The benefits of using MRI
Types of endometriomas not detectable by ultrasound but by MRI include cells located on tendons.
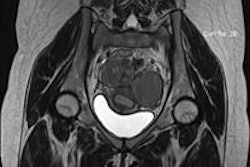
 Axial T1-weighted image of a 29-year-old woman with bilateral endometriomas. All images courtesy of Dr. Julia Wenzel.
Axial T1-weighted image of a 29-year-old woman with bilateral endometriomas. All images courtesy of Dr. Julia Wenzel. A sagittal T2-weighted image of a 32-year-old woman with endometrial lesions of the Douglas pouch as well as the posterior bladder wall.
A sagittal T2-weighted image of a 32-year-old woman with endometrial lesions of the Douglas pouch as well as the posterior bladder wall.An additional benefit of MRI is that the surgeon does not need to be present for the patient examination, which is the case for ultrasound; he/she can analyze the images independently before the intervention.
MRI proved to be particularly reliable in the detection of endometriomas in the rear abdominal cavity and, with a detection rate of 90%, on the colon. This is significant because endometrial tissue is frequently overlooked in that region. In a number of cases, endometriomas grow into the colon wall and are difficult for the surgeon to see.
The method was somewhat less successful for the front abdominal cavity, in particular for the bladder and the uterine wall. MRI proved less helpful in detecting very small endometriomas.
 A 25-year-old woman with endometrial lesions of the rectosigmoid colon. Sagittal T2-weighted image showing a hyperintense nodule infiltrating the sigmoid wall.
A 25-year-old woman with endometrial lesions of the rectosigmoid colon. Sagittal T2-weighted image showing a hyperintense nodule infiltrating the sigmoid wall.Benefits of utilizing MRI include the fact that, for cysts, the technology shows metabolites, allowing to identify the age of the cysts and to differentiate endometrial from other types of cysts.
The recommendation
In cases where the decision has been made in favor of medication therapy influencing hormones, ultrasound is a suitable option.
 Axial T2-weighted image of a thickened right uterosacral ligament in a 42-year-old patient.
Axial T2-weighted image of a thickened right uterosacral ligament in a 42-year-old patient."However, the study demonstrates that preceding interventions, MRI is to be recommended for the planning of surgical interventions for all patients with endometriosis," Wenzel summarized. "MRI helps the surgeon to detect the lesions and increases the chances for the patient to find herself symptom free after intervention."