Infant body weight has been given precedence over infant age in the Republic of Ireland, where a new diagnostic reference level standard (DRLS) is being developed to define radiation exposure limits from mobile chest x-ray performed in the country's neonatal intensive care services.
Newborns requiring intensive care -- or special baby care, as it is referred to in the Republic of Ireland -- often undergo multiple chest x-rays. Though individual chest x-ray procedures involve limited radiation exposure, the effects of additional studies are cumulative. The possibility of induced cancers over a lifetime for such young patients has raised alarms for some physicians and public health officials.
"It is important to have reference standards to guide optimization of relatively low-dose procedures that may be performed frequently on newborn infants," said Kate Matthews, a radiographer and director of quality at the University College Dublin School of Medicine and Medical Science.
Matthews and Mark McEntee, PhD, a lecturer in diagnostic and biological imaging at the same institution, presented their findings at the 2011 ECR. McEntee has also been involved with CT diagnostic reference dosing projects in Portugal and Malta.
Diagnostic reference levels standards that vary from 0.53 to 1.35 cGy*cm² depending on patient weight were recommended for chest radiography performed on infants who are less than a year old. They will be forwarded to the Irish public health service for possible national adoption following peer-reviewed publication, Matthews wrote in response to written questions from AuntMinnieEurope.com.
The standards are based on radiation dose-area product (DAP) measures acquired in 2004 from 64 mobile x-ray chest exams on newborns and infants at six randomly selected hospitals that represent a cross-section of facilities providing neonatal intensive care unit (ICU) services in the country.
To ensure reproducibility, a single DAP meter was transferred from hospital to hospital to capture dose readings from all mobile chest exams performed on neonates and infants at each institution for a two-week period.
The investigators followed methods from the Commission of European Communities (CEC) to calculate the reference level standards. The CEC instructed researchers to survey a range of practices, rather than relying on data from a few specialized, high-volume centers, Matthews wrote.
The mean DAP dose at each hospital was ranked for infants who were younger than 1 month old and from 1 month to 1 year old. Using CEC methods, Matthews and McEntee calculated the DRLS at the 75th percentile level was 0.8 cGy*cm² for both age groups. (Centigray, as a product of cm², signifies the dose in the air kerma multiplied by area of exposure, thereby accounting for the effects of collimation and source-to-image distance.)
"This result concerned us slightly as we believed that the 75th percentile dose should have been lower for the neonatal group," Matthews wrote. "So, we grouped the babies by weight and again looked at the dose distribution."
Linear relationship by weight
That action revealed a linear relationship between DAP and weight, with the lowest dose usually associated with smallest babies, she noted.
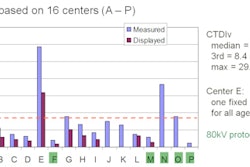
The resulting diagnostic reference level guidelines were plotted on the following six-point scale depending on infant weight:
Radiation exposure for mobile chest x-ray performed on neonates and infants
|
||||||||||||||
| Data courtesy of Kate Matthews. | ||||||||||||||
The values compare favorably with published reference values, according to Matthews. They typically range between 0.3 and 0.8 cGy*cm² without accounting for infant weight.
Radiation variations uncovered
The study found DAP for individual exams varied within and between hospitals by factors of up to 17 and 24, respectively, but no more than a fivefold variation in mean dose was observed between hospitals, Matthews said. Small sample sizes for infants at specific weights may have contributed to the variation.
The survey found that field-of-view, kVp, and mAs settings had the greatest influence on DAP, with higher DAP readings associated with combinations of lower kVp and high mAs values, Matthews said.
The highest readings were associated with computed radiography (CR). CR tended to use the lowest kVP and highest mAs settings in combination. CR's accrued DAP dose was 4.7 times higher than mobile x-ray systems, which were associated with the lowest doses.
"This isn't saying there is anything inherently bad about CR systems, or indeed any other receptor system," Matthews said. "Just that it is important when introducing a new receptor to investigate the optimal combinations of kVp and mAs from a dose perspective, as well as for image quality."
Ultimately, diagnostic reference level standards establish a benchmark encouraging practitioners to reduce radiation exposures, according to Matthews. The published literature indicates repeat audits following the publication of a DRL will reduce the amount of variation in radiation dosages within and between facilities.
The Matthews-McEntee survey carries the bonus of data demonstrating the need adjust x-ray system setting for the infants weight.
"We hope the importance of using baby weight to determine exposures beyond the neonatal period is recognized and adopted into practice," she said.



![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnieeurope.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&fit=crop&h=100&q=70&w=100)





![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnieeurope.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)






