A multidisciplinary group in the U.K. has released a free-to-download 18-page document about the practical aspects of running a successful CT colonography (CTC) clinic and planning for the future.
The key components necessary for CTC services should include increased scanner provision, appointment of CTC service managers, appropriate training of a multidisciplinary workforce, local leadership teams monitoring and developing CTC services, and formation of collaborative networks to share local expertise and training opportunities and to coordinate delivery of services, according to the report.
"The number of diagnostic tests needed to exclude colorectal cancer will substantially increase over the next decade," the authors noted. "As the demands on colonoscopy services increase with expansion of bowel cancer screening and surveillance programs, it is likely that CTC provision will need to increase substantially to provide the necessary capacity for investigation of symptomatic patients."
The main 14 recommendations are as follows:
- CTC services should produce a quality assurance report every three years.
- CTC services should use structured report templates for reporting all examinations using the format indicated in the Bowel Cancer Screening Services database.
- CTC services should comply with the recommended service benchmarking and audit guidance.
- Postimaging colorectal cancer cases should be analyzed using the World Endoscopy Organisation framework.
- CTC services must have a named lead radiologist and lead radiographer accountable to the clinical director with responsibility for all aspects of service delivery and adherence to quality assurance standards.
- Lead radiologists and lead radiographers should have allocated leadership time for service development, training, audit, and quality assurance in addition to their clinical workload.
- CTC services require radiologists, radiographers, administrative, pharmacy, and medical physics professionals to provide quality-assured CTC services.
- New or expanding CTC services should use a workforce calculator to determine future staffing requirements for sustainable quality-assured services.
- Collaborative networks should be developed between trusts to share local expertise, training opportunities, and delivery of services.
- A national cloud-based CTC quality assurance portal should be created to evaluate and improve CTC service performance that is integrated with national databases and regional radiology networks.
- A national CTC training and accreditation program for radiographers and radiologists should be commissioned to support and monitor training.
- A curated national cloud-based CTC case repository should be developed for training and accreditation in interpretation.
- CT scanner capacity must be increased to allow expansion of CTC services.
- Regional networks should link to designated centers of excellence responsible for delivering CTC education and training.
 Proposed pathway flow diagram for lower gastrointestinal investigation. Courtesy of RCR.
Proposed pathway flow diagram for lower gastrointestinal investigation. Courtesy of RCR.CTC is a first-line test for the exclusion of colorectal cancer and large polyps in patients with symptoms suggestive of bowel cancer, the authors wrote. They stated that CTC is also indicated for the following:
- Incomplete colonoscopy performed for new symptoms suggestive of colorectal cancer and for colorectal surveillance.
- Patients with abdominal symptoms requiring extracolonic evaluation in addition to colonic assessment.
- Patients with significant comorbidities increasing the risk of colonoscopy who require investigation of new symptoms suggestive of colorectal cancer and who need colorectal surveillance.
- Previous failed colonoscopy where a repeat attempt is considered unlikely to be successful.
- Patient choice/colonoscopy refusal in symptomatic patients where appropriate counseling is provided.
"Decision-making when selecting the most appropriate test for a patient relies on a full appreciation of the requirements for both colonoscopy and CTC," they pointed out.
In the case of England, other components should be data submission from all National Health Service (NHS) facilities for audit against published standards, commissioning a national CTC training and accreditation program for radiographers and radiologists performing or interpreting CTC, they recommended.
The authors also advocate funding a national cloud-based CTC case interpretation repository for training and accreditation, as well as funding a national cloud-based CTC quality assurance portal to evaluate performance in those already trained and accredited. Other important aspects are research funding prioritization to improve patient risk stratification and investigation triage to maximize patient flow, diagnostic yield and productivity, and effective pretest triage with widely available and nationally standardized fecal immunochemistry test (FIT) testing, they noted.
About the report
Overall, the document outlines the key components required of CTC services to meet the needs of patients and clinicians in primary and secondary care and highlights the referral pathways, quality assurance, leadership, organization, and resource requirements necessary to deliver a better patient experience and outcomes. Its intention is to outline the necessary components to build a uniform provision of high-quality CTC services across the NHS in England for patients.
The report was compiled by a multidisciplinary group of 19 experts from radiology, radiography, Gastroenterology, and colorectal surgery across England. It represents a collaboration between the British Society of Gastrointestinal and Abdominal Radiology (BSGAR), the Royal College of Radiologists (RCR), the Society and College of Radiographers (SCoR), the Gastro Intestinal Radiographers Special Interest Group (GIRSIG), and other stakeholders, including the National CT Colonography Training and Accreditation Programme and the Association of Coloproctology of Great Britain and Ireland (ACPGBI).
To download a free copy of the document, go to the RCR website.
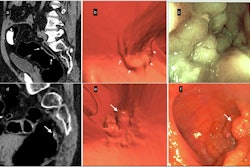
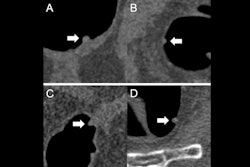
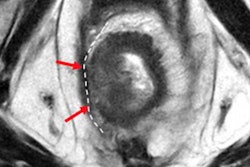
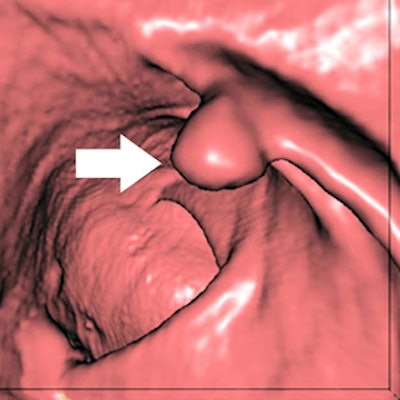
Editor's note: the image used to introduce this article on the homepage is a CTC of a 9-mm polyp (arrow) in the descending colon of a 78-year-old woman. Virtual fly-through 3D reconstructions were used for exact polyp localization. Courtesy of Dr. Sergio Grosu and colleagues from Ludwig Maximilian University of Munich and the RSNA.