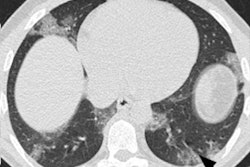
French researchers have found that chest CT is an effective tool for initial diagnosis of COVID-19, according to a study published on 1 September in Radiology. The results challenge current guidelines that have discouraged initial use of CT for COVID-19.
Most COVID-19 guidelines recommend that CT not be used to screen for the disease, suggesting that clinicians first rely on reverse transcription polymerase chain reaction (RT-PCR) testing, wrote a team led by Dr. Guillaume Herpe of University Hospital Center Poitiers. But not only does RT-PCR testing take longer to process than a CT exam, it can also produce false negatives.
"In the context of this epidemic, the low sensitivity of RT-PCR implies that many patients with COVID-19 may not be identified and consequently may not be isolated from healthy population," the authors wrote. "These individuals could continue to spread this disease. Chest CT can detect some characteristic features in almost all patients with COVID-19 pneumonia ... [including] patients with clinical symptoms but negative RT-PCR results but with clinical symptoms."
Chest CT's role and performance in diagnosing COVID-19 has been debated since the pandemic began, with some experts -- including the American College of Radiology (ACR) and the Fleischner Society -- actually discouraging its routine use for screening or suggesting that it be used only in patients with severe symptoms. But everyone agrees that rapid diagnosis of COVID-19 is crucial.
"It is essential to detect this disease at its earliest stage and immediately isolate the infected person to limit its spread," the authors noted.
Herpe's team sought to assess the efficacy of chest CT and RT-PCR testing for COVID-19 using final discharge diagnosis as the reference standard. The team sent a survey regarding the use of CT to diagnose COVID-19 between 2 March and 24 April -- the peak of France's experience of the pandemic -- to 26 French hospital radiology departments.
The survey asked respondents to include all asymptomatic patients suspected of having COVID-19 who underwent both chest CT and at least one RT-PCR test within 48 hours of presentation at the hospital. All 26 departments responded to the survey, which included data from 4,824 eligible patients.
Of these patients, 2,564 (53%) were positive for COVID-19 disease. CT performed well among the patient cohort, the group found. Of note, in 103 patients with an initial positive CT for COVID-19 who then had a negative initial RT-PCR test, a repeat RT-PCR test was positive in 90%.
| Chest CT, RT-PCR performance for diagnosing COVID-19 | ||
| Measure | CT | RT-PCR |
| Accuracy | 90% | 97% |
| Negative predictive value | 89% | 87% |
| Positive predictive value | 92% | 99% |
| Sensitivity | 90% | 87% |
| Specificity | 91% | 99% |
Herpe and colleagues also discovered that, in patients with both negative CT and RT-PCR, negative predictive value of presence of COVID-19 using the combination of the two tests was 99%.
The study findings fly in the face of previous recommendations, according to the authors.
"[Our] results ... shed light on the role of chest CT in the current COVID-19 pandemic as an initial diagnostic tool in areas of relatively high disease prevalence," they concluded.