When radiologists use strong, specific follow-up recommendations in FDG-PET/CT reports, referring physicians are more likely to follow their advice -- and find cancers, according to a Dutch study published online on July 29 in the Journal of the American College of Radiology.
In a review of nearly 2,500 reports from clinical FDG-PET/CT scans performed over an 18-month period at their institution, researchers from the radiology department at University Medical Center Groningen in the Netherlands found that strongly worded recommendations for follow-up radiological or nonradiological exams significantly increased the rate by which referring physicians adhered to the advice. What's more, follow-up exams performed following these recommendations led to a malignant diagnosis in a substantial number of cases, according to lead author Dr. Hasan Alesawi and colleagues.
To gauge the strength of the radiologist's follow-up recommendations, the researchers searched the reports for keywords such as "recommended," "advised," "may be considered," or "if clinically indicated." In addition, they also searched for more specific guidance, such as "additional MRI" and "gynecological consultation," as well as guidance suggesting a nonspecific course of action, including terms that included "further evaluation indicated" or "follow-up required."
Of the 2,496 FDG-PET/CT reports, 193 (8%) included general recommendations for follow-up. Referring physicians, however, acted only on 120 (62%) of those recommendations. Of the reports in which the recommendations were followed, 21 (17%) resulted in a malignancy diagnosis for patients. As for the 73 recommendations that were not followed, three (4%) patients were diagnosed with a cancer.
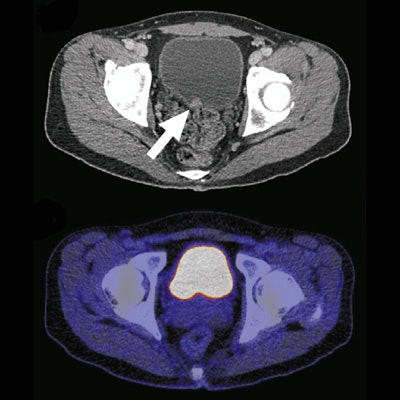
 A 40-year-old man with plasmablastic lymphoma and multiple bone lesions underwent FDG-PET at baseline (A) and six months later (B). CT shows a focal hyperdense lesion at the bladder floor (C, arrow) that is not clearly visible on fused FDG-PET/CT (D). The FDG-PET/CT report included a strong recommendation for focused ultrasonography to evaluate the bladder lesion. However, the referring physician disregarded the recommendation for unclear reasons. Six months later, the patient presented with hematuria, and cystoscopy showed a bladder tumor, which was removed by transurethral resection (E, arrow). Images courtesy of JACR.
A 40-year-old man with plasmablastic lymphoma and multiple bone lesions underwent FDG-PET at baseline (A) and six months later (B). CT shows a focal hyperdense lesion at the bladder floor (C, arrow) that is not clearly visible on fused FDG-PET/CT (D). The FDG-PET/CT report included a strong recommendation for focused ultrasonography to evaluate the bladder lesion. However, the referring physician disregarded the recommendation for unclear reasons. Six months later, the patient presented with hematuria, and cystoscopy showed a bladder tumor, which was removed by transurethral resection (E, arrow). Images courtesy of JACR."Interestingly, the recommendations that were followed by the referring physicians led to a specific malignant diagnosis significantly more frequently than recommendations that were disregarded," the authors wrote. The difference was statistically significant (p = 0.006).
Alesawi and colleagues suggested that this result could be due to referring physicians having "more clinical information and can better judge the clinical relevance of perceived or potential lesions than reporting imaging physicians." It's also possible, based on the lack of dedicated follow-up exams in those patients, that the outcome of disregarded recommendations could be not be determined significantly more frequently than the outcome of recommendations that were followed, according to the authors.
Regarding the strength of words and terms in follow-up recommendations, the researchers tallied 157 reports (81%) with specific courses of action, compared with 36 reports (19%) with no specific guidance. Strong wording and the frequency of follow-up actions were significantly associated (p = 0.019) with the referring physicians' compliance with the recommendations in the FDG-PET/CT reports (odds ratio of 2.14).
"Therefore, nuclear medicine physicians and radiologists should pay attention to this part of the communication in the FDG-PET/CT report, particularly when dealing with a critical finding on the FDG-PET/CT scan," the researchers concluded.
The authors noted that their study was conducted at a single tertiary care academic medical center. Thus, "results may not be applicable in private practice settings," they wrote.