A Swiss study has shown that a CT protocol using tin filtration and iterative reconstruction reduces radiation dose levels to the equivalent of a chest x-ray for lung volumetry and also the detection and quantification of emphysema. The results nudge ultralow-dose CT ever closer to routine workup of chest pathologies.
Because the technique's radiation dose levels are comparable with conventional x-ray examinations, ultralow-dose CT may substitute for chest x-ray in certain scenarios, opening a wide field of clinical applications, according to the research group from the University Hospital of Zurich and Cantonal Hospital of St. Gallen.
However, the authors point to the importance of studying and validating the technique's diagnostic value for the detection and classification of each different disease individually (European Journal of Radiology, June 2017, Vol. 91).
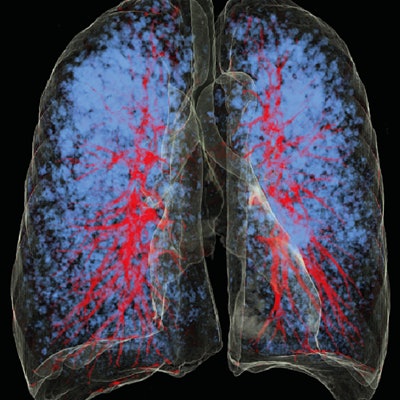
 CT images of the lung in a 48-year-old woman with emphysema. She had a body mass index of 17.6 kg/m2, and was scanned with standard dose (left column) and ultralow dose (right column). Low attenuation areas (LAA) in blue represent emphysematous lung changes. The extent and distribution of emphysema is equally recognizable in chest x-ray equivalent ultralow-dose at 0.14 mSv CT compared with standard dose CT. All images courtesy of Dr. Michael Messerli.
CT images of the lung in a 48-year-old woman with emphysema. She had a body mass index of 17.6 kg/m2, and was scanned with standard dose (left column) and ultralow dose (right column). Low attenuation areas (LAA) in blue represent emphysematous lung changes. The extent and distribution of emphysema is equally recognizable in chest x-ray equivalent ultralow-dose at 0.14 mSv CT compared with standard dose CT. All images courtesy of Dr. Michael Messerli.The authors note CT has become one of the most widely used tools for evaluating the lung parenchyma, and chest CT enables reliable detection of pulmonary emphysema, the end-stage destruction of the lung parenchyma. On CT, low attenuation areas (LAA) -- where the lungs contain pure air -- represent emphysema, which can be detected by automated measurement of the areas in the lung that are below a certain density (< -950 HU).
At the same time, there is ongoing debate over the potentially harmful effects of CT radiation. Techniques have been developed to reduce CT radiation dose, such as using a tin filter for spectral shaping of the 100-kV x-ray source spectrum, which eliminates low-energy quanta that mainly contribute to patient dose but not to image generation.
Another tool is the use of iterative reconstruction techniques rather than standard filtered back projection (FPB) to reconstruct CT data. When used in combination with the tin filter technique, iterative reconstruction can achieve "drastic dose reduction," as low as 0.13 mSv -- about the level of a chest x-ray.
But the applicability of these new techniques for emphysema quantification and lung volumetry have not been analyzed, the authors note. The researchers therefore decided to use the ultralow-dose technique to measure lung volumes and quantify the amount of emphysema in patients prior to surgery, and compare the findings with standard-dose CT.
 CT images of the lung in a 27-year-old man with a body mass index of 20.6 kg/m2. He was scanned, after spontaneous pneumothorax, with standard dose (left column) and ultralow-dose (right column). LAA in blue represent paraseptal emphysema (zoomed in right upper lobe). The extent and distribution of emphysema is equally recognizable in chest x-ray equivalent ultralow-dose at 0.14 mSv CT compared with standard dose CT.
CT images of the lung in a 27-year-old man with a body mass index of 20.6 kg/m2. He was scanned, after spontaneous pneumothorax, with standard dose (left column) and ultralow-dose (right column). LAA in blue represent paraseptal emphysema (zoomed in right upper lobe). The extent and distribution of emphysema is equally recognizable in chest x-ray equivalent ultralow-dose at 0.14 mSv CT compared with standard dose CT.In the prospective study, 84 consecutive patients from a single center underwent clinically indicated standard-dose chest CT (1.7 ± 0.6 mSv). Of the 84 patients, 40 (48%) had no emphysema, and 44 (52%) had emphysema.
The ultralow-dose protocol used single-energy ultralow-dose CT (0.14 ± 0.01 mSv) at 100 kV and fixed tube current at 70 mAs with tin filtration. The team used a commercially available iterative reconstruction technique (advanced modeled iterative reconstruction, ADMIRE, Siemens Healthineers).
The study revealed that increasing levels of ADMIRE resulted in a decrease of emphysema values (LAA) both in standard dose and ultralow-dose CT. Also, software-based LAA values, which are higher in ultralow-dose CT compared with standard dose CT, can be partially corrected with higher strength levels of iterative reconstruction (IR), the authors stated.
| Overview of the LAA% values | ||
| FBP standard dose | Ultralow-dose CT | |
| LAA% | 4.4 | |
| ADMIRE 3 | 2.6 | 5.7 |
| ADMIRE 4 | 2.1 | 4.1 |
| ADMIRE 5 | 1.8 | 2.4 |
 LAA values of (a) all patients (b) patients with no emphysema and (c) patients with emphysema. Overall LAA values are much higher in emphysema patients.
LAA values of (a) all patients (b) patients with no emphysema and (c) patients with emphysema. Overall LAA values are much higher in emphysema patients.Specifically, the median LAA using filtered back projection in standard-dose was 4.4%. This decreased to 2.6%, 2.1%, and 1.8% using ADMIRE 3, 4, and 5, respectively. The median values of LAA in ultralow-dose CT were 5.7%, 4.1%, and 2.4% for ADMIRE 3, 4, and 5, respectively. There was no statistically significant difference between LAA in standard-dose CT using FBP and ultralow-dose using ADMIRE 4 (p = 0.358) as well as in standard-dose CT using ADMIRE 3 and ultralow-dose using ADMIRE 5 (p = 0.966).
Emphysema detection and quantification was feasible at a radiation dose equivalent to chest x-ray, but using ADMIRE led to"underestimation" of emphysema volumes compared with standard filtered back projection data reconstruction. No significant differences were seen in emphysema measurements between standard-dose and ultralow-dose CT using ADMIRE.
However, because there was still variation between the techniques, it is unclear whether ultralow-dose CT provides sufficient precision to detect disease progression in follow-up examinations. They recommend performing longitudinal CT analyses with fixed dose levels, same scan protocol, and reconstruction algorithms for reproducibility.
Feasibility studies needed
Lead author Dr. Michael Messerli, a resident in the nuclear medicine department at the University Hospital of Zurich, noted the current study is part of a series the group is conducting in ultralow-dose CT with a third-generation dual-source scanner using a tin filter for spectral shaping of the 100 kV x-ray source spectrum, which eliminates low-energy quanta that mainly contribute to patient dose but not to image generation.
"This study confirms the evolving value of ultralow-dose techniques for detecting and characterizing different pathologies of the chest," Messerli told AuntMinnieEurope.com.
He highlighted how the extent and distribution pattern of emphysema can be easily visualized using these techniques. Furthermore, because the level of LAA is a strong independent predictor of mortality, CT quantification can also help identify subgroups of patients with chronic obstructive pulmonary disease.
"Early stratification may enable targeted therapies and research based on individual CT phenotypes," Messerli noted.
However, he cautioned that emphysema values tend to be "overestimated" in ultralow-dose CT and that the use of iterative image reconstruction can lead to a variation of emphysema volume.
The group is now validating ultralow-dose CT protocols for assessing other pathologies such as coronary calcifications, an important risk predictor for cardiovascular morbidity.
"We encourage other researchers to evaluate x-ray-dose-equivalent CT protocols within clinical studies to critically appraise the feasibility of routine implementation of ultralow-dose CT, establish where it can substitute chest x-ray with an incremental diagnostic value, and evaluate its cost-effectiveness in different clinical settings and healthcare systems," Messerli said.
Senior author Dr. Ralf Bauer, consultant radiologist specializing in dual-source CT and professor of radiology at the Cantonal Hospital St. Gallen, added it was now down to radiologists to evaluate which clinical referrals were suitable for ultralow-dose -CT protocols and to evaluate and ensure that with stronger IR settings relevant pathologies will not be missed.
"So far, we have been able to clearly evaluate x-ray-dose-equivalent CT for lung nodule detection, which is a major step toward a broad-based utilization of CT for lung cancer screening. We need to further focus on dedicated clinical questions and patient groups to find the ideal scenario and individual patient to benefit from these technical developments,"he concluded.