
Thanks to 3-tesla MRI, radiologists can now measure coronary flow velocity reserve (CFVR), noninvasively showing the significance of CT-detected stenosis in all three major arteries, researchers from Japan reported at last month's ECR 2014 in Vienna.
Measuring coronary flow velocity reserve with MRI is a proven option for assessing the significance of a coronary stenosis noninvasively, but until now its utility has been limited.
"Phase-contrast cine MRI (PC-MRI) can provide noninvasive assessment of coronary flow velocity reserve by measuring coronary arterial flow at rest and during hyperemia," said Dr. Takatoshi Higashigawa from Matsusaka Central Hospital in Japan. "However, CFVR measurement with 1.5-tesla MR systems has been limited to the LAD (left anterior descending) artery."
Now, improved signal-to-noise ratios using high-field 3-tesla MRI may allow reliable flow quantification in the right coronary artery (RCA) and left circumflex artery (LCX), he said.
The goal of the research was to determine if PC-MRI at 3-tesla can provide accurate detection of altered CFVR caused by significant stenosis in the three major coronary arteries including LAD, LCX, and RCA, he said.
Higashigawa and colleagues from Matsusaka Central Hospital, along with Dr. Masake Ishida and colleagues from Mie University Hospital in Japan, enrolled 16 patients (mean age 71 ± 9 years) prospectively between May and August 2013.
All patients were scheduled for invasive coronary angiography due to suspicion of obstructive coronary artery disease at coronary CT angiography (CCTA), which found at least one moderate stenosis in a vessel 2.5 mm or larger, Higashigawa said.
In all, the research team examined 27 coronary arteries at CCTA, including seven with stenosis (RCA 7, LAD 11, LCX 2) and seven normal arteries (RCA 4, LCX 7).
After acquiring the cine MRI sequences, 3D respiratory-gated coronary MRI was performed on a 3-tesla scanner (Ingenia, Philips Healthcare). Then phase-contrast MRI was acquired during rest and adenosine triphosphate stress.
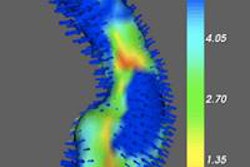
"We used multiplanar reformation of whole-heart coronary MR angiography to determine the double oblique imaging plane that is perpendicular to the target vessel," he said. The PC-MRI acquisitions were obtained at a location distal to the stenosis.
Phase-contrast MRI was performed using a single breath-hold acquisition and the following parameters:

CFVR assessment was completed in 25 of 26 (96%) cases.
The study team used CVi42 software by Circle for image analysis, manually tracing the contour of each artery, Hagashigawa said. They performed background corrections by means of regions of interest placed on adipose tissue adjacent to the coronary artery.
CFVR was calculated as the maximum velocity during hyperemia divided by maximum velocity at rest. Thus, for a peak velocity increase from 7 to 22 cm per second in one case, the resulting CFVR was three, Hagashigawa said.

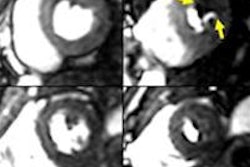
In this case, CCTA showed a stenosis in the RCA. Flow measurement in the distal RCA demonstrated a CFVR of 2.0, suggesting no significant stenosis. The diameter stenosis at quantitative coronary angiography was 45%.
This slide shows relationship between percent coronary stenosis on quantitative coronary angiography (QCA) and CFVR on phase-contrast MRI. Moderate inverse correlation (y = -0.022x + 2.9, r = -0.57, p = 0.002) was found between coronary stenosis at QCA and CFVR.

Moreover, the intraclass correlation coefficient between CFVR measurements by two observers was 0.82, showing a good interobserver reproducibility.
"CFVR measurements in LCX and RCA as well as LAD seem to be quite reasonable," Hagashigawa said.
The group also looked at the diagnostic performance of 3-tesla phase-contrast MRI for detecting significant coronary stenosis at QCA by ROC curve analysis; they found high diagnostic performance with an area under the curve (AUC) of 0.89, he said. Sensitivity of 83%, specificity of 85%, positive predictive value of 63%, and a high negative predictive value were also noted.

"Phase-contrast MRI at 3 tesla can provide noninvasive detection of altered CFVR in three major coronary arteries with significant stenosis," Hagashigawa concluded. "CFVR measurement by PC-MRI at 3 tesla seems to be useful for ruling out physiologically significant coronary stenosis in patients with suspected CAD [coronary artery disease] on coronary CT angiography."

















![A normal mammogram confirmed by three-year radiologic follow-up illustrates reader-marked regions of interest (ROIs) during (A) unaided (round 1) and (B) artificial intelligence (AI)–assisted (round 2) reading. Each colored dot represents an ROI for recall by a human reader. Readers could mark more than one ROI per case, represented by multiple dots of the same color. During AI-assisted reading, the AI system displayed three visible prompts: two with suspicion of malignancy scores of 35% (left mediolateral oblique [L MLO] and craniocaudal [L CC]) and one with a suspicion of malignancy score of 10% (right craniocaudal [R CC]), shown as polygonal overlays. Without AI, six of 10 readers (60%) marked a false-positive ROI. With AI assistance, this fell to two of 10 (20%). R MLO = right mediolateral oblique.](https://img.auntminnieeurope.com/mindful/smg/workspaces/default/uploads/2026/07/2026-07-14-radiology-mammogram-ai-auto-bias.H0bYO8QlWs.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)