When it comes to breast ultrasound, combining B-mode, Doppler techniques, and elastography can help improve true-positive and true-negative diagnosis results by reducing the operator's influence on the outcome, according to an Austrian expert.
"We have to apply new algorithms and bring them together to more or less create the best algorithm we can offer," said Dr. Christian Weismann from the diagnostic and interventional breast department at St. Johanns Hospital in Landeskliniken Salzburg.
In the near future, ultrasound frequencies for breast ultrasound will not increase considerably, he noted. The broadband ultrasound transducer (e.g., 5-16 MHz) with dynamic adaption of different frequency bands is standard.
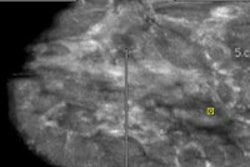
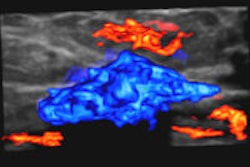
 Invasive ductal carcinoma of the breast viewed using real-time 4D tissue elastography technique. Image courtesy of Dr. Ako Itoh of the department of surgery at Hitachi General Hospital in Ibaraki, Japan.
Invasive ductal carcinoma of the breast viewed using real-time 4D tissue elastography technique. Image courtesy of Dr. Ako Itoh of the department of surgery at Hitachi General Hospital in Ibaraki, Japan."Standardization is an important topic, especially for the future, because many companies are providing medical devices, and each company has a different access or way to present this information," Weismann commented during the recent World Federation for Ultrasound in Medicine and Biology (WFUMB) congress in Vienna.
Radiologists have to strike a balance between ultrasound artifacts and penetration, but to assist them, improved spatial and contrast resolution can be combined with high computer power and computer-aided detection (CAD) software. Also, tissue harmonic imaging improves contrast and reduces artificial, low-level echoes in the cyst lumen. A potential problem, however, is to misinterpret a cyst-like solid lesion as a cyst.
"In the future, ultrasound CAD will be established routinely," he said. "BI-RADS assessment of a lesion will be performed by CAD software, and instantly the BI-RADS classification will be offered by the computer."
In the near future, an automated optimization of the frequency band following the individual tissue properties will be a step toward standardization of ultrasound imaging. Additionally, CAD will influence the image result in order to have a perfect basis for automated lesion analysis.
"If you think of a mammogram, you can show it to a radiologist in Chicago or Sydney and they can both read it," Weismann said. "This is one of the big topics or issues: to standardize the information in a way that we all have the same settings, the same results."
The slow blood-flow sensitivity of color Doppler systems will detect flow velocities far less than 1 cm/sec, combined with improved suppression of ultrasound artifacts, he predicted. Also, accurate comparability of 3D color datasets for the follow-up of breast lesions, such as before and after neoadjuvant chemotherapy, is extremely helpful.
"Ultrasound is a little bit like driving a car," Weismann said. "You have to do it yourself and you have to read it. But if you had the option for a 3D dataset to cover the entire breast, then I would accept that a technician or sonographer or whoever obtains the 3D dataset. And you get the full information afterward. You can read this additional ultrasound and there is no need to recall the patient for examination."
Doppler also offers improved ultrasound-contrast enhancers for contrast harmonic imaging, he added.
A benefit of using elastography is there is no freehand compression and decompression at the body surface. Moreover, propagation of shear waves happens in 1 to 10 m/sec.
"From my point of view, the shear wave access is the one with the highest level of standardization," Weismann said. "If you compare this with compression and decompression and you study the results afterward, it is always a problem if the individual has a strong influence on the result or outcome. You can reduce this if there is no need to compress or decompress but only to keep the transducer stable in position in the region of interest. This is a very strong point for standardization."
Also, tissue elasticity is directly measured in kPa. Not to mention it is independent of user skill. In the future, analysis of elasticity will be offered by CAD, he pointed out.
Combining all three techniques will optimize the BI-RADS assessment and improve the true-positive and true-negative computer results. The end game is to reduce the operator's influence on the diagnostic outcome.
"These are rather simple things, but they will have an extremely strong impact on our future," Weismann concluded.