The largest multicenter study ever undertaken in France to establish the clinical value of coronary CT angiography (CTA) in stable patients delivered good sensitivity for detecting coronary artery disease (CAD), according to a presentation at the 2011 ECR.
At the same time, specificity was on the low side, investigators said, possibly owing to the generous inclusion criteria that included even patients with heavy coronary artery calcifications and prior stenting. But overall image quality was good, and coronary CT angiography was particularly useful for detecting coronary artery disease in patients at intermediate risk.
In recent years a number of multicenter trials have sought to assess the clinical value of coronary CTA, however, few have included more than 1,000 patients, said Jean-Pierre Laissy from Hôpital Bichat Claude-Bernard in Paris.
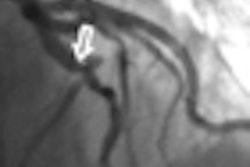
Laissy and colleagues from 40 centers throughout France examined the diagnostic performance of coronary CTA compared with invasive coronary angiography.
"We needed a population of more than 1,000 patients in order to have an idea of the value of MDCT," Laissy said in his presentation.
Between June 2006 and June 2008, the researchers prospectively enrolled 1,254 symptomatic patients who underwent MDCT angiography less than four days before elective coronary angiography.
Following exclusion of 192 patients, 153 of whom did not complete one of the two exams, the researchers analyzed the results in 1,062 patients (4,248 segments and 16,297 segments) assessed by both modalities. Blinded visual analysis of the results was performed by experienced readers in independent core labs, and statistical analysis was performed per patient, per vessel, and per segment, he said.
In all, 73.9% of the scanners were equipped with 64-detector-rows or more, while about 26% were 16-detector-row scanners. The predominant manufacturer was GE Healthcare; the company provided 51% of the scanners used in the trial.
"Since the studies were retrospective we had higher levels of radiation exposure (18.2 mSv ± 7.9 ) compared to previous studies," Laissy said. The prevalence of coronary artery disease (> 50% stenosis) was 52.3%, with 40.5% of patients presenting with single-vessel disease, 31.7% with two-vessel disease, and 27.8% with three-vessel disease, Laissy said. The distribution was as follows: left anterior descending 36.3%, right coronary artery 30.1%, circumflex artery 26.7%, and left main artery 3.5%. The mean reading time was 28 ± 12 minutes.
The final study population constituted 1,048 patients. Image quality was excellent or good in 41.4% of patients, "and when the technical quality was good or fair (55.9%) it was mainly due to heart motion artifacts," Laissy said.
Motion artifacts were responsible for average or fair image quality in 41% of patients, followed by insufficient vascular enhancement in 17%, image noise in 14%, and breathing artifacts in 7%, he said.
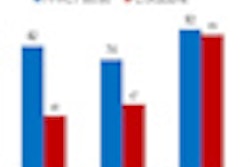
Performance analysis of coronary CTA in 1048 patients
|
||||||||||||||||||||
| PPV = positive predictive value; NPV = negative predictive value |
"The results are different between different populations, with very low PPV, but good NPV in the low-probability population, and conversely high sensitivity and moderate PPV and NPV in the high-probability population," Laissy said.
Diagnostic performance per patient according to risk levels (Duke score)
|
Overall the prevalence of coronary artery disease was 52%, and the NPV of coronary CTA for ruling out significant stenosis was 84% -- demonstrating high sensitivity but only moderate specificity, Laissy said.
The methodologic choice of considering all vessels that were inaccessible at CT as stenosed probably led to underestimation of the clinical efficacy of coronary CTA -- considering that at conventional angiography, 85.4% of these segments were either normal or had stenoses of less than 50%, he said.
"When we compared our results with [those of] other multicenter trials, we found that our NPV was quite bad, but the PPV was quite similar to the concurrent publications," Laissy said.
The results show that coronary CTA has clinical value in documenting the coronary tree and particularly for the assessment of patients at intermediate risk of coronary artery disease, he said. Understanding the diagnostic accuracy of MDCT in this population of patients can be used to aid the establishment of clinical application guidelines, he said.
"The results we obtained are results that we can see clinically every day in our practice," Laissy said. "Probably since there are more than 1,000 patients ... we will be able to use this database to perform studies in the group of patients with CABG [coronary artery bypass grafts], patients with stents, women against men, and so on," he said.