CT is a game changer for emergency diagnoses of the elderly, but radiologists must take great care not to confuse normal age-related changes with the cause of the emergency, delegates heard at the French national radiology congress, JFR, on 5 October.
Experts at the session -- called “Elderly patients in the emergency room: better understanding for better imaging” and moderated by Dr. Ingrid Millet from Montpellier University Hospital (CHU Montpellier) -- provided tips and advice on how to perform and interpret high-quality CT scans. They also discussed the ethical considerations related to the constant growth in imaging demand, which is sometimes out of step with therapeutic possibilities for this population.
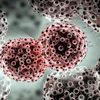
![Inappropriate chest CT angiography protocol. Investigation of pulmonary embolism in a 73-year-old man. Left: False pulmonary embolism (red arrow) due to incomplete opacification caused by premature acquisition of the pulmonary artery (OG empty of contrast [yellow arrow]). Right: After a new injection with a later start of acquisition, correct filling of the branches of the pulmonary artery. All images courtesy of Drs. Ingrid Millet, Catherine Cyteval, Gilbert Ferret, Patrice Taourel, and Mathieu Lederlin and presented at JFR 2025.](https://img.auntminnieeurope.com/mindful/smg/workspaces/default/uploads/2025/10/2025-10-06-jfr-imaging-of-elderly-fig-1.buWU7nYfJR.jpg?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) Inappropriate chest CT angiography protocol. Investigation of pulmonary embolism in a 73-year-old man. Left: False pulmonary embolism (red arrow) due to incomplete opacification caused by premature acquisition of the pulmonary artery (OG empty of contrast [yellow arrow]). Right: After a new injection with a later start of acquisition, correct filling of the branches of the pulmonary artery. All images courtesy of Drs. Ingrid Millet, Catherine Cyteval, Gilbert Ferret, Patrice Taourel, and Mathieu Lederlin and presented at JFR 2025.
Inappropriate chest CT angiography protocol. Investigation of pulmonary embolism in a 73-year-old man. Left: False pulmonary embolism (red arrow) due to incomplete opacification caused by premature acquisition of the pulmonary artery (OG empty of contrast [yellow arrow]). Right: After a new injection with a later start of acquisition, correct filling of the branches of the pulmonary artery. All images courtesy of Drs. Ingrid Millet, Catherine Cyteval, Gilbert Ferret, Patrice Taourel, and Mathieu Lederlin and presented at JFR 2025.
While people over the age of 75 currently represent around 10% of the population, they accounted for more than 16% of emergency room visits in 2024, an increase of 5% compared with 2023, according to the FEDORU 2025 report. Their stay in the emergency room is longer than other age groups due to the complexity of their conditions, which require additional tests, and is even longer when hospitalization is considered, which accounts for 48% of cases, noted the JFR presenters in an article published in SFR Actu on 5 October.
Numerous studies have shown that clinical and biological data are unreliable and insufficiently discriminating to guide these patients correctly, and any delay in diagnosis leads to increased morbidity in the elderly. Therefore, imaging, particularly CT scans, plays a central role in the emergency department in establishing an accurate diagnosis. However, radiologists must distinguish between normal age-related signs and truly significant pathologies, they explained.
Fractures often manifest themselves through subtle, atypical, and even misleading signs in elderly patients, noted Dr. Catherine Cyteval, a specialist in osteoarticular imaging at Lapeyronie Hospital, CHU Montpellier. She highlighted how osteoporosis, spinal deformities, and osteoarthritis further complicate the interpretation of examinations.
Particular vigilance is required, she continued. Radiologists must monitor the bone cortices in the three planes, carefully examine soft tissue windowing, and use MRI if there is any doubt, she urged. Interventional radiology, particularly cementoplasty, also plays a key role in promoting a rapid return to physical activity and preventing slippage syndrome.
 Unstable T11 fracture in a stiff spine in a 92-year-old osteoporotic patient (arrow). The patient had a history of cementoplasty of L1 and L2.
Unstable T11 fracture in a stiff spine in a 92-year-old osteoporotic patient (arrow). The patient had a history of cementoplasty of L1 and L2.
Dr. Gilbert Ferret, a chest imaging specialist from CHU Grenoble Alpes, detailed the expected age-related changes in the various anatomical compartments of the chest: subpleural reticular patterns, increased bronchial-arterial ratio, and thickening of the bronchial wall.
Scans performed in cases of suspected pulmonary embolism have a lower diagnostic yield in this population, but often allow differential diagnoses to be identified, according to Ferret. He underlined the technical adjustments required to obtain a high-quality CT angiogram, while flagging the importance of allowing time to obtain patient cooperation.
Abdominal imaging specialist Dr. Patrice Taourel, also from Lapeyronie Hospital, CHU Montpellier, illustrated the frequent discrepancy between the lack of clinical signs and the severity of lesions revealed by imaging, particularly in cases of intra-abdominal inflammation or infection.
He revealed how certain specific or common pathologies warrant particular care, and these included tumor-induced colonic obstruction, the leading cause of intestinal obstruction, and digestive ischemia affecting the small intestine, colon, or gallbladder. Furthermore, in cases of right upper quadrant pain, extra-abdominal causes such as pneumonia or myocardial infarction should not be underestimated, he noted.
Communication between radiologists, geriatricians, surgeons, and emergency physicians remains key to rapid and safe care, ensuring both diagnostic accuracy and a better care pathway for older patients, the JFR speakers concluded.