Evidence is mounting that low-dose 3D contrast-enhanced MR angiography (CE-MRA) is both practical and reproducible in the carotids, chest, abdomen, and lower extremities, and may reduce the risk of dose-dependent patient complications.
"I think the future is low-dose contrast-enhanced MRA," Dr. Kambiz Nael, from the department of radiological sciences, David Geffen School of Medicine, University of California at Los Angeles, told AuntMinnieEurope.com. "We have already implemented this in our routine clinical practice here at UCLA. We can perform CE-MRA for a variety of anatomic regions, including supra-aortic, pulmonary, abdominal, and distal runoff, sometimes using as little as 7 cc of [gadolinium] contrast. I believe with more improvement in hardware and software, we may be able to lessen the contrast dose even further if needed."
In a review article in the October issue of the European Journal of Radiology, the UCLA team explored the current utilization and experience with contrast dose reduction in CE-MRA, as well as factors that affect its success (Vol. 80:1, pp. 2-8). They also share how time-resolved MRA techniques may ultimately be a viable alternative in patients at elevated risk of nephrogenic systemic fibrosis (NSF).

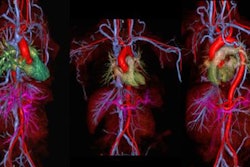
 A 45-year-old woman experienced a transient ischemic attack. Coronal anterior inverted MIP (left) and posterior oblique volume-rendered (right) images from a high spatial resolution CE-MRA. The examination was performed by distributing a multiple array of coils over a large FOV (450 mm) to cover the entire supra-aortic arteries from the aortic arch to the vertex on a 3-tesla MR system. After IV injection of 0.1 mmol/kg (approximately 8 ml), the entire 3D dataset was obtained with isotropic voxel size of 0.8 mm³ during acquisition time. Note segmental irregularity and beaded appearance of the cervical segment of the left internal carotid artery compatible with fibromuscular dysplasia. All images courtesy of Dr. Kambiz Nael.
A 45-year-old woman experienced a transient ischemic attack. Coronal anterior inverted MIP (left) and posterior oblique volume-rendered (right) images from a high spatial resolution CE-MRA. The examination was performed by distributing a multiple array of coils over a large FOV (450 mm) to cover the entire supra-aortic arteries from the aortic arch to the vertex on a 3-tesla MR system. After IV injection of 0.1 mmol/kg (approximately 8 ml), the entire 3D dataset was obtained with isotropic voxel size of 0.8 mm³ during acquisition time. Note segmental irregularity and beaded appearance of the cervical segment of the left internal carotid artery compatible with fibromuscular dysplasia. All images courtesy of Dr. Kambiz Nael."The higher the baseline [signal-to-noise ratio], the more the potential for contrast dose reduction, so that 3-tesla field strength, multichannel RF architecture and high relaxivity contrast agents may support aggressive dose reduction strategies," the authors wrote. "Attention to detail in contrast infusion and image acquisition protocols is mandatory for reproducibility and quality control. Finally, time-resolved MRA with ultralow-dose contrast is likely to play an important role in patients at elevated risk of NSF."
While CE-MRA is widely utilized for assessment of almost all vascular territories, the use of high-dose gadolinium (Gd) agents -- and the linkage of these agents with NSF in renal failure patients -- has led to concerns over the safety of this technique. As a result, contrast dose reduction techniques are being explored.
Although contrast dose reduction can be costly in terms of signal-to-noise ratio (SNR), recent experience suggests that significant redundancy has been built into Gd dosage protocols and these have entered into widespread clinical practice, the authors noted. A number of approaches can reduce contrast dose, including the use of higher field strength.
Since higher field strengths such as 3-tesla yield higher SNR, this can be used to cut acquisition time and/or improve spatial resolution. In addition, sensitivity to injected gadolinium contrast for CE-MRA is further heightened as the longitudinal relaxation time of unenhanced blood increases with field strength. This supports the potential for dramatic dose reductions in comparison with conventional 1.5-tesla protocols.
For both 1.5-tesla and 3-tesla, further improvement in imaging quality and performance has been realized by the debut of more sensitive imaging coils and multiple receiver channels, according to the authors. Even more aggressive parallel imaging protocols are now possible, thanks to continued development of coil arrays and multiple receive channels. The combination of this advanced RF technology and SNR gains from higher-field scanners can also offset any potentially deleterious effects from contrast dose reduction in CE-MRA, stated the UCLA researchers.
Extended field-of-view imaging may also add value in situations where pathology extends beyond the coverage of a single body array coil, such as in thoraco-abdominal aortic aneurysms or aortic dissections that extend above and below the diaphragm.
"The only penalty for such extended coverage is a higher demand on machine computing power; an increasingly insignificant limitation with modern processors and inexpensive computer memory," they wrote.
Injection protocol
Since contrast infusion protocols for lower-extremity CE-MRA are crucial determinants of study quality, modifications must be carefully designed, according to the authors. The UCLA uses approximately 0.2 mmol/kg Gd total dose at 1.5-tesla and approximately 0.1 mmol/kg at 3-tesla.
"Relative to the older, higher dosage protocols, we implemented the reduced dosage protocols by diluting the native Gd formulation with normal saline, while maintaining the original infusion volume," the authors wrote. "This enables use of the exact same infusion rates of the diluted contrast as of the original full strength contrast, so that no changes are required in timing of the acquisition. If the contrast agent is not diluted, the volume of injected contrast solution must be decreased proportionately to the dose reduction."
Anecdotal experience has found that reliability of timing injections may be compromised at injection rates below 1 ml/s, as Gd may simply pool in an arm vein, the researchers reported. As a result, the institution dilutes the contrast by the same factor as the required Gd dose reduction and maintains the original infusion rate.
"So, for example, if the original protocol involved injecting 30 ml Gd at 2 ml/s for carotid MRA at 3-tesla and if we require a four-fold reduction in contrast dose, we dilute the Gd formulation to quarter strength and infuse 30 ml of quarter strength Gd solution at 2 ml/s; the dose equivalent of 7.5 ml undiluted Gd formulation," they pointed out. "This has, in fact, been our routine practice for carotid CE-MRA at 3-tesla for over three years."
The researchers added that image quality can be maintained when employing a similar approach to performing high-spatial-resolution CE-MRA of the lower extremity arterial tree with a contrast dose in the order of 0.1 mmol/kg.
"Our low-dose protocols have been robust over the past three years and have likely diminished the risk of dose-dependent complications," the authors noted.
Time-resolved MRA
Thanks to parallel acquisition and sparse k-space sampling methods, time-resolved MRA (TR-MRA) can now produce high frame-rate 4D images that offer visualization of blood flow temporal dynamics, according to the researchers. And TR-MRA also requires only very small doses of Gd.
"Although the specifics of protocol and contrast dose may vary depending on the clinical application, our TR-MRA protocols generally employ very low contrast doses (on the order of 2-6 ml)," they wrote. "In the light of recent discussions of NSF, many practices have seen TR-MRA as a viable alternative to conventional CE-MRA in patients at elevated risk of NSF."
At UCLA, TR-MRA is commonly used to evaluate arteriovenous malformations, to evaluate anatomic and post-surgical shunts in patients with congenital heart disease, and to assess central venous occlusive disease.
"The growing population of patients with end stage renal disease and their increased survival has substantially increased the burden associated with their related complications including diagnoses and management of central venous occlusive disease," the authors wrote. "TR-MRA has potential as an initial and follow-up diagnostic tool and may obviate the need for conventional CE-MRA in this high risk population."