Using routine clinical protocols in whole-body FDG-PET/CT, Danish researchers have found that a point spread function (PSF) PET reconstruction technique increases lesion detection for numerous cancers, according to an article in press published by the European Journal of Radiology.
Researchers from Copenhagen University Hospital believe the additional information provided by PSF-based PET image reconstruction could enhance diagnosis and staging of cancers and help evaluate therapy response (EJR, 17 December 2012).
Lead study author is Dr. Flemming Littrup Andersen from the hospital's department of clinical physiology, nuclear medicine, and PET. The group prospectively evaluated 41 consecutive patients who were referred for a clinical whole-body PET/CT examination using FDG. Clinical indications for staging or restaging included 15 cases of gynecological cancers, eight patients with lymphomas, three people each with mesothelioma and melanomas, two individuals each with lung cancer and sarcomas, and eight forms of other cancers.
The patient cohort included 10 males with a mean age of 48 years, ranging from 15 to 68 years of age, and 31 females with a mean age 60 years, ranging from 23 to 87 years of age.
Imaging protocols
All whole-body scans were done on a four-ring lutetium oxyorthosilicate-based PET/CT system (Biograph 40 TruePoint, Siemens Healthcare) after patients fasted for six hours prior to injection of 400 (± 40) MBq of FDG.
The whole-body PET/CT acquisition included a spiral CT scan and PET data were acquired in 3D mode at 2.5 minutes per bed position. CT images were reconstructed with a 70-cm field-of-view and a 3-mm slice thickness. PET data were corrected for scatter and attenuation using acquired CT images prior to PET image reconstruction.
Researchers evaluated two PET image reconstruction protocols based on attenuation-weighted ordered subset expectation maximization (AW-OSEM). The first method was a standard AW-OSEM (referred to as R1 in the study) and AW-OSEM with the PSF-model (referred to as R2).
An experienced nuclear medicine physician evaluated the reconstructed attenuation-corrected (AC) PET images and was blinded to the two image reconstruction protocols (R1 or R2). The PET images were given randomly to the physician with a minimum of two weeks between reconstructions (R1 or R2) of the same patient.
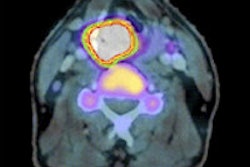
 Whole-body PET/CT shows the difference between AW-OSEM (left) and AW-OSEM with PSF (right) and the increase in SUVmax by adding PSF. Image courtesy of Dr. Søren Holm.
Whole-body PET/CT shows the difference between AW-OSEM (left) and AW-OSEM with PSF (right) and the increase in SUVmax by adding PSF. Image courtesy of Dr. Søren Holm.The reader graded the overall image quality of the whole-body AC-PET images on a five-point scale, with 1 as "very poor" and 5 as "very good." The physician also tallied the number of visible lesions from the AC-PET images based on anatomical regions, such as the head and neck, mediastinum, lungs, liver, spleen, abdomen, pelvis, bones, and other areas.
The researchers also conducted a volume of interest analysis on a sample of 58 lesions, which were visible in both image sets. The review included the most prominent lesion activity as seen on AC-PET and a 3D rendering marked the lesion.
Image quality
The evaluations for mean overall quality of the AC-PET images was 4.2 (± 0.6) for R1 and 4.3 (± 0.7) for R2 with the difference between the two techniques deemed not statistically significant.
Researchers also counted 91 PET-positive lesions using the standard AW-OSEM reconstruction (R1) technique, compared with 103 PET-positive lesions with AW-OSEM PSF model (R2). The authors concluded the difference was statistically significant.
No lesions were detected in 12 (29%) of 41 patients by either R1 or R2 techniques. There were 17 (41%) patients in whom all lesions seen on both R1 and R2.
Standard reconstruction found three lesions not detected on R2 in three cases (7%). However, PET image reconstruction with PSF (R2) detected a total of 15 lesions in nine (22%) that were not seen on R1.
The study also noted that lesions were located within a minimum of 5 mm and a maximum of 139 mm from the center of the field-of-view and the smallest and largest lesions were 4 mm and 44 mm in diameter, respectively. Lesion volumes decreased by a minimum of 2% and a maximum of 79% with the R2 technique, with the exception of one lesion.
Based on the results, Andersen and colleagues concluded this study proved a "significant effect" of iterative image reconstruction using the spatial image resolution model on clinical PET image quality and quantification.
"We observed an increase in PET-positive lesions, as well as a significant change in the measured SUV [standardized update volume] and volumes of these lesions," the authors wrote. "These quantitative changes may impact diagnosis and staging, as well as therapy response assessments depending on the algorithm chosen. Therefore, standardized imaging protocols are encouraged for intra- and interpatient analysis."