The input and knowledge of radiologists is proving invaluable in diagnosing pelvic and upper thigh problems in football players. Imaging is also contributing extensively to the management of weightlifting and bodybuilding injuries.
"A footballer's pelvis, hips, and thigh muscles are subjected to a great deal of strain with turning, quick acceleration and deceleration, and of course kicking," noted Dr. Cleofina Furtado, a radiology trainee at University Hospitals of North Midlands NHS Trust in Stoke-on-Trent, U.K., and Dr. Rania Zeitoun, a musculoskeletal imaging specialist at Kasr Al-Ainy School of Medicine, Cairo University.
Injuries in these players are common and frequent. Many patients are managed conservatively, as in the case of low-grade muscle strain or tendon sprain, and imaging might not be needed. In more serious and chronic injuries, imaging is essential for appropriate management, they explained.
 Biceps femoris muscle tear in a 35-year-old male footballer. (a) Axial T2-weighted fat-saturated, (b) Sagittal T2-weighted, and (c) Coronal T2-weighted fat-saturated MRI of pelvis demonstrates interstitial edema within the long head of the biceps femoris muscle (white arrowheads) with an area of fluid-signal intensity (white curved arrow). Note the interruption of the muscle and intramuscular tendon, representing muscle laceration reaching the medial myofascial surface. All images courtesy of Dr. Cleofina Furtado, Dr. Rania Zeitoun et al, and EPOS/European Society of Radiology (ESR).
Biceps femoris muscle tear in a 35-year-old male footballer. (a) Axial T2-weighted fat-saturated, (b) Sagittal T2-weighted, and (c) Coronal T2-weighted fat-saturated MRI of pelvis demonstrates interstitial edema within the long head of the biceps femoris muscle (white arrowheads) with an area of fluid-signal intensity (white curved arrow). Note the interruption of the muscle and intramuscular tendon, representing muscle laceration reaching the medial myofascial surface. All images courtesy of Dr. Cleofina Furtado, Dr. Rania Zeitoun et al, and EPOS/European Society of Radiology (ESR)."Pelvic apophyseal injuries are common in young football players," stated Furtado and Zeitoun. "Apophyses, bony attachments of the tendons, are a common site of acute avulsion secondary to forceful muscle contraction. This might affect the anterior superior iliac spine, anterior inferior iliac spine, ischial tuberosity, iliac crest, and pubic bones, as well as the greater and lesser trochanters of the femur."
Surgery is usually considered in cases of significantly displaced avulsion fracture. In chronic nonunion avulsion fracture, deformities, pseudoarthrosis, and more serious complications like impingement might be encountered necessitating surgical correction.
Continuous muscle traction exerts stress on the growing bone, resulting in chronic forms of injuries like in ischial apophysitis and osteitis pubis, they continued. These chronic injuries are a source of chronic pain that might affect training and generate concern, especially in young players at the start of their career.
"X-ray is good at demonstrating bone changes in chronic cases, while MRI is more helpful demonstrating bone edema at the anatomical site of tendon attachment and further revealing aponeurotic, tendon, and myotendon injuries," the researchers pointed out.
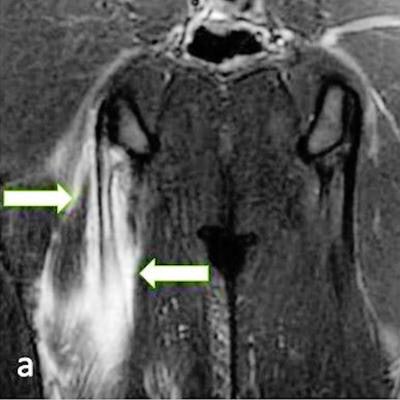
 23-year-old male footballer with right semimembranosus muscle longitudinal split tear. (a) and (b) Coronal T2-weighted fat-saturated MRI of pelvis shows feathery edema in bipennate muscle fibers (arrows) converging on central tendon (white solid arrows). This demonstrates longitudinal split, with the proximal extent of tear extending almost up to the level of ischial tuberosity (white dashed arrow).
23-year-old male footballer with right semimembranosus muscle longitudinal split tear. (a) and (b) Coronal T2-weighted fat-saturated MRI of pelvis shows feathery edema in bipennate muscle fibers (arrows) converging on central tendon (white solid arrows). This demonstrates longitudinal split, with the proximal extent of tear extending almost up to the level of ischial tuberosity (white dashed arrow).Muscle injuries are frequent in football players, mostly in hamstrings, quadriceps, adductors, and calf muscles. Ultrasound is a helpful primary imaging modality, but MRI remains the mainstay in the diagnosis of muscle injuries, identifying precise anatomical location and pattern of injury that might range from interstitial edema without fibers distortion to more severe injury pattern with fibers and architecture distortion, laceration, and gap. The injury might involve one or more of these components: muscle fibers, myoaponeurosis/fascia, myotendinous junction, and tendon.
"Intramuscular degloving of the rectus femoris is a pattern of injury associated with kicking where dissociation of the inner (indirect head) and outer (direct head) muscle layers result in bull's eye appearance on MRI," they added.
Additionally, myositis ossificans traumatica is a posttraumatic complication affecting the muscles or tendons, commonly of the pelvic girdle and lower limbs of football players. "This might occur following a major trauma or repeated microtraumas, presenting with pain (possibly intense in acute stage), discomfort, restricted muscle function or impingement syndromes. They are classified among the 'don't touch lesions.' "
Internal hip joint derangement with labrum tear and cartilage damage can result in early osteoarthritis.
Weightlifting and bodybuilding injuries
Radiologists also play an important role in accurate assessment and early diagnosis of commonly encountered soft tissue and bone injuries in the shoulder girdles and arms of weightlifters, allowing for better functional and aesthetic outcomes, according to Furtado and Zeitoun.
In weightlifting, there are two key events: the snatch and the clean and jerk. "Technical errors, fatigue, overloading, and dropping weights are associated with injury. A wide variety of soft tissue and bone injuries might be encountered."
The acromioclavicular joint is subjected to repeated microtrauma and increased stress to the subchondral bone on the distal clavicular side, predisposing to subchondral fractures and distal clavicular osteolysis. Acromioclavicular joint cartilage damage and accelerated osteoarthritis might follow, they pointed out.
"Radiographs help to show more advanced stages with distal clavicular cortical erosions and joint space widening. The superiority of MRI is in demonstrating early and occult abnormalities before becoming evident on x-ray. Fluid-sensitive sequences show bone edema while T1-weighted imaging is better at showing cortical erosions and subchondral fractures."
Repeated arm lifting results in continuous friction and perhaps impingement of the rotator cuff tendons in the subacromial tunnel, the authors noted. Subacromial bursitis and various forms of supraspinatus tendinopathies and often tears are encountered as a result in weightlifters. Ultrasound and MRI are helpful in allowing accurate evaluation of the size and extent of these tears.
 After lifting weights at the gym, a 33-year-old man presented with a partial articular supraspinatus tendon avulsion (PASTA) with superior labral anterior posterior (SLAP) tear. Coronal T1 and T1-weighted fat-saturated MRI arthrogram demonstrates a Type II SLAP tear; contrast entered the space between the superior labrum, with both vertical and horizontal component insinuating anteriorly towards the biceps tendon (straight white arrows). The biceps tendon is intact (yellow curved arrow). Also, note the PASTA lesion with tendon failure on the articular side of the supraspinatus tendon (red arrow).
After lifting weights at the gym, a 33-year-old man presented with a partial articular supraspinatus tendon avulsion (PASTA) with superior labral anterior posterior (SLAP) tear. Coronal T1 and T1-weighted fat-saturated MRI arthrogram demonstrates a Type II SLAP tear; contrast entered the space between the superior labrum, with both vertical and horizontal component insinuating anteriorly towards the biceps tendon (straight white arrows). The biceps tendon is intact (yellow curved arrow). Also, note the PASTA lesion with tendon failure on the articular side of the supraspinatus tendon (red arrow)."Flexing the shoulder into an extreme overhead position increases the risk of injury-causing shoulder instability," they wrote. "Different types of labrum injuries have been previously reported including superior labral anterior posterior (SLAP) tears, anterior and posterior glenohumeral instabilities with subsequent impaired function besides the persistent pain that hinders adequate training and practice."
MR arthrography is helpful in delineating labral tear extent and pattern, capsulolabrum and ligaments attachments, and cartilage integrity.
Although rare in the general population, "pec tears" (pectoralis major rupture) are relatively common in weightlifters and bodybuilders, the authors wrote. The injury is commonly incomplete rupture of the myotendinous junction of the sternal head. A complete tear of its tendinous attachment is less common. MRI is excellent at diagnosing these injuries considering optimizing the field-of-view and acquisition angles to fully visualize the muscle and its tendon.
 A 27-year-old man presented with a pectoralis major muscle injury, following a weight-training session in the gym. (a) Axial, (b) Coronal, and (c) Sagittal STIR images. Partial tear is visible at the myotendinous junction (black arrowhead and circle), mostly involving the sternal head with muscle fiber retraction. Edema is noted at the distal muscle fibers (white dashed arrow) but no complete tears. Preserved common tendon insertion at the humerus (red arrow).
A 27-year-old man presented with a pectoralis major muscle injury, following a weight-training session in the gym. (a) Axial, (b) Coronal, and (c) Sagittal STIR images. Partial tear is visible at the myotendinous junction (black arrowhead and circle), mostly involving the sternal head with muscle fiber retraction. Edema is noted at the distal muscle fibers (white dashed arrow) but no complete tears. Preserved common tendon insertion at the humerus (red arrow).Rupture of the biceps tendon is more common, and proximal rupture of the long-head tendon has also been reported. "Both ultrasound and MRI are helpful in determining biceps rupture, whether partial or complete, tendon retraction, the presence of hematoma, myotendinous junction, and muscle belly and importantly assessment of associated injuries like rotator cuff tendon or labrum tears."
In active athletes, continuous sliding movement of the scapula over the rib cage result in soft tissues irritation at the scapulothoracic space that might manifest as bursitis, they noted. "A subsequent audible or palpable click might be encountered in what is described as 'snapping scapula syndrome.' The latter also includes various underlying anatomical and mechanical etiologies encompassing variations in the anatomy of the scapula bone, periscapular muscles dyskinesia, and space-occupying lesions."
To view the authors' e-poster about football injuries, go to the EPOS section of the ESR's website. To view their weightlifting exhibit, click here. The co-authors of the e-posters were Dr. P. Venkatappa and Dr. S. Yousry Gamal Bakr.



















