Laxative-free CT colonography (CTC) now rivals the results obtained with a conventional cathartic bowel preparation. A large series performed with only low-dose iodinated contrast fecal tagging was highly accurate for detecting polyps 6 mm and larger, and was well accepted by patients, according to a new Spanish study published online by European Radiology.
Performed on nearly 2,000 average-risk screening subjects, the largest study to date according to the authors, noncathartic CTC achieved a positive predictive value (PPV) of 94% for lesions 6 mm and larger.
The main advantage of using high-osmolarity iodine contrast medium at low doses is that it both softens stools and tags them with few collateral effects, producing a homogenous mixture that facilitates interpretation, wrote Dr. Carmen Zueco Zueco and colleagues from Complexo Hospitalario Universitario de Vigo in Pontevedra, Spain. The formula reduces the side effects of traditional cathartic CTC, which goes a long way toward improving the patient experience, they added.
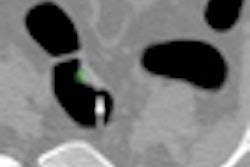
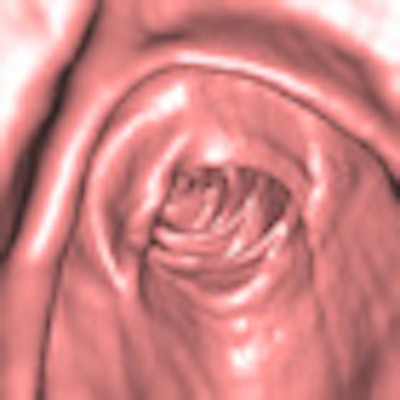
 A 58-year-old woman at average risk of a colorectal neoplasm, who was asymptomatic. Left: 3D endoluminal image shows a 20 mm flat polyp (protruding less than 3 mm from the mucosa). Histology confirmed an adenocarcinoma located in the ascending colon (arrow). Right: 2D axial image confirms that the polyp identified in (left) is a soft-tissue lesion (arrow). Axial image shows no residual fluid in left and right colon (score 5). Score of 4 and 5 in sigmoid (arrowhead) for quantity and tagging residual fluid. Distension score of 5 in the whole colon. Image courtesy of Dr. Carmen Zueco Zueco.
A 58-year-old woman at average risk of a colorectal neoplasm, who was asymptomatic. Left: 3D endoluminal image shows a 20 mm flat polyp (protruding less than 3 mm from the mucosa). Histology confirmed an adenocarcinoma located in the ascending colon (arrow). Right: 2D axial image confirms that the polyp identified in (left) is a soft-tissue lesion (arrow). Axial image shows no residual fluid in left and right colon (score 5). Score of 4 and 5 in sigmoid (arrowhead) for quantity and tagging residual fluid. Distension score of 5 in the whole colon. Image courtesy of Dr. Carmen Zueco Zueco."The essential factor is to achieve good-quality colon cleansing and tagging of residual stool, which guarantees accuracy in the diagnosis, permitting its use in a real clinical setting," Zueco and colleagues wrote (Eur Radiol, 13 January 2012). The study aimed to determine the positive predictive value of CTC performed without cathartic preparation for polyps 6 mm or larger and assess overall patient experience.
The study included 1,920 average-risk patients (1,191 women and 729 men; mean age 64.4) referred for CTC over a three-year period. Additionally, the first 700 patients completed two self-administered questionnaires, the first before CTC to assess preparation discomfort, and the second after the exam to assess the distress associated with the exam.
Fecal tagging was performed via oral administration of 60 mL of diatrizoate meglumine and diatrizoate sodium with an iodine concentration of 370 mg/mL (Gastrografin, Schering, Berlin) over 42 hours. Patients followed a low-fiber diet the first day and added 7.5 mL of the contrast with three meals on the second day. The third day the 7.5-mL contrast dose accompanied a liquid diet, along with at least 2 L of water each day.
On the day of the exam, manual colonic insufflation with room air was performed. Prone and supine CTC images were acquired on a 16-detector-row scanner (Somatom, Siemens Healthcare) using 16 x 0.75-mm collimation, 1-mm slice thickness, 0.7-mm reconstruction increment, 25 mAs, and 100 kV.
Images were interpreted by one of two experienced radiologists on a workstation (Wizard with syngo colonography software, Siemens) using a primary 3D interpretation technique with 2D problem-solving. Fiber-optic colonography was performed on patients with CTC-detected polyps or masses within 92 days following a positive CTC exam. Lesion measurement was performed using a visual comparison and used for polyp matching with the CTC results.
In all, 14.9% (n = 287) of the 1,920 patients had at least 1 polyp 6 mm or larger in diameter, with 125 patients having at least one polyp 10 mm or larger, the authors reported. A total of 20 false-positive polyps 6 mm or larger were found in 14 patients at CTC, for a false-positive rate of 5.9%.
The results showed a per-polyp positive predictive value of 95% to 98% for lesions ranging from 6 mm to larger than 30 mm, with an overall per-patient PPV of 92.8%.
PPV and false-positive rate for noncathartic CTC vs. optical colonoscopy in CTC-positive patients
|
"The high overall per-patient PPV, 92.8% at the 6-mm size threshold, reflects a very good agreement in positive findings between CTC and subsequent OC [optical colonoscopy]," Zueco and colleagues reported. "This result is in line with recent previous studies in clinical practice with conventional preparation with laxatives showing a 90% to 92% PPV," and substantially outperforms Pickhardt and colleague's landmark 2003 trial (New England Journal of Medicine, 4 December 2003), they said, noting that a high PPV is an important attribute for CTC in as much as it protects against unnecessary additional diagnostic exams.
"It could be argued that in a clinical practice setup, where false-negative rates cannot be assessed, high PPV could result from only truly relevant lesions being detected," Zueco and colleagues noted. "However, out of 236 patients who underwent OC after positive CTC findings, only in 10 (4.2%) were diagnosed additional polyps not previously detected by CTC."
In all, 7.4% of patients reported diarrhea on a day in which Gastrografin was ingestion, with all but 12 describing symptoms as mild, with 7.6% reporting abdominal discomfort. The preparation caused minimal discomfort for 78.9% of patients and was severely unpleasant for 2.9%. The overall CTC experience was rated minimally unpleasant for 55% of patients and severely unpleasant for 6%.
Of the 33 false-positive and false-negative polyps reported, five were due to differences in localization and six to size differences that broke the polyp matching rules, the group noted.
The 8.7% rate of advanced neoplasia, slightly higher than that of other trials, may be due to a slightly older population (mean age 64.4 years). "However, this can be taken as an indication that relative performance of CTC is not lessened when no cathartics are used in patient preparation," the group wrote. Adenocarcinoma was detected in one 6- to 9-mm lesion (0.8%), in 22 lesions 1 mm or larger (20.2%), and 26 masses 3 cm or larger (56.5%), with the authors also attributing those higher than average rates to higher mean patient age compared with other screening studies.
Some 86% of patients had liquid feces, believed to facilitate interpretation. "Since residual stool is generally recognized as a major source of potential error at CTC, the scarce fecal residue, either liquid or solid, along with the excellent labeling achieved with the iodine fecal tagging preparation in our study are remarkable results, especially so given the small volume of iodine applied with regard to that used in other studies," Zueco and colleagues wrote, adding that the long 42-hour Gastrografin administration probably helped optimize the tagging results.
"CTC without cathartic bowel preparation and iodinated agents for fecal tagging can obtain high PPV values and a low rate of false-positive results for ≥ 6-mm polyps comparable to those obtained with conventional preparation with laxatives," the researchers concluded. "Furthermore, because of a good patient experience, this method could really improve the acceptance of CTC for colorectal cancer screening."