The danger of stroke as a cardiac postsurgery complication has flagged the need for greater understanding of patients' calcified atherosclerotic burden prior to surgery. But just how much dose is needed for CT results to be accurate, and how can radiologists optimize visualization? Swiss researchers have investigated.
CT can reliably quantify thoracic aortic calcification, and several studies have suggested preoperative CT in cardiac surgery may reduce postoperative stroke rate by altering surgical strategy and obviating heavy manipulation of the aorta. However, because of the potentially harmful effects of radiation exposure from CT, minimizing dose remains a priority if the modality is to be used in routine practice.
A group from Zürich aimed to determine the value of ultralow-dose chest CT for estimating atherosclerotic burden of the thoracic aorta using tin-filter technology and to compare its diagnostic accuracy with chest x-ray. In the study published online on 3 October in British Journal of Radiology, the team revealed that the technique provides a reliable estimation of burden at x-ray equivalent dose and also showed its diagnostic accuracy was significantly higher than that of x-ray.
"Preoperative assessment of aortic atherosclerotic burden with minimum radiation dose might prove valuable for patients undergoing cardiac or aortic surgery by optimizing the surgical approach and decreasing aortic plaques related to postoperative complications," lead author Dr. Michael Messerli, a resident in the nuclear medicine department at the University Hospital of Zürich, told AuntMinnieEurope.com. "To our knowledge, this is the first in vivo study investigating the value of modern tin-filter CT for assessing the thoracic atherosclerotic burden at dose levels in the range 0.1 - 0.15 mSv, similar to a conventional chest x-ray."
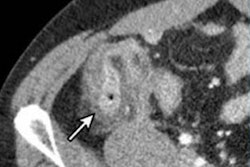
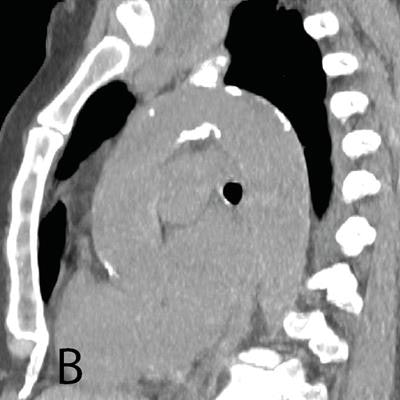
 A: Representative posteroanterior chest x-ray image. B, D, and E: Transverse CT sections scanned with standard-dose CT (effective dose 1.57 mSv). C, F, and G: Ultralow-dose CT (effective dose 0.12 mSv) in an 83-year-old woman with a body mass index of 26.1 kg m2. As the images illustrate, ultralow-dose CT allows for anatomically differentiated assessment, with a high agreement of calcium quantity estimation of the aortic valve, ascending aorta, and aortic arch as compared with standard-dose CT. Image courtesy of BJR and Dr. Michael Messerli et al.
A: Representative posteroanterior chest x-ray image. B, D, and E: Transverse CT sections scanned with standard-dose CT (effective dose 1.57 mSv). C, F, and G: Ultralow-dose CT (effective dose 0.12 mSv) in an 83-year-old woman with a body mass index of 26.1 kg m2. As the images illustrate, ultralow-dose CT allows for anatomically differentiated assessment, with a high agreement of calcium quantity estimation of the aortic valve, ascending aorta, and aortic arch as compared with standard-dose CT. Image courtesy of BJR and Dr. Michael Messerli et al.Their study included a total of 106 patients, 43 (41%) women and 63 (59%) men, from a prospective single-center study. In the same session, these patients underwent standard-dose chest CT with 110 kV (1.7 ± 0.7 mSv) by clinical indication followed by ultralow-dose CT with 100 kV and spectral shaping by a tin filter (0.13 ± 0.01 mSv) to achieve an equivalent dose to chest. All scans were conducted on a third-generation dual-source CT scanner (Somatom Force, Siemens Healthineers).
Two independent radiologists reviewed the images, rated image quality, and estimated the presence and extent of calcification of the aortic valve, ascending aorta, and aortic arch. X-rays also were included if they were performed within three months from the time the CT study was conducted and if both posteroanterior and lateral views were available (n = 49; 46% of study group). If no chest x-ray was available in this time period (n = 57; 54% of study group), an x-ray mimic was created via a thick multiplanar reformation in both views from the CT dataset of the ultralow-dose scan.
Each image was rated on a five-point Likert scale for its diagnostic value for calcifications, a rating of 1 attributed to poor image quality and low diagnostic value, while a rating of 5 indicated images of excellent quality and high diagnostic value. The extent of calcification for each localization was categorized as being absent, minimal, mild, moderate, or severe.
Significant results
The images of 106 patients, including standard-dose CT, ultralow-dose CT, and chest x-rays, yielded a total of 318 datasets. The researchers found that the sensitivity for detecting thoracic aortic calcification was significantly lower on chest x-ray (52.5%) compared with ultralow-dose CT (p < 0.001).
The key findings are shown below, with sensitivity and specificity percentages for plain chest x-ray and ultralow-dose CT, along with confidence interval (CI), for detecting thoracic aortic calcifications and standard-dose CT as the reference.
| Diagnostic performance of plain chest x-ray & ultralow-dose CT | |||||
| Chest x-ray | Ultralow-dose CT | ||||
| Parameter | Aorta | Aortic valve | Ascending aorta | Aortic arch | p-value* |
| Sensitivity (%, CI) |
52.5% (41.0-63.8) |
93.5% (78.6-99.2) |
96.2% (87.0-99.5) |
96.2% (89.3-99.2) |
< 0.001 |
| Specificity (%, CI) |
69.2% (48.2-85.7) |
97.3% (90.7-99.7) |
100% (93.3-100.0) |
92.6% (75.7-99.1) |
< 0.001 |
Furthermore, in terms of the value of ultralow-dose CT for estimation of calcifications, the researchers found a high agreement for calcium quantity estimation between standard-and ultralow-dose CT images with weighted p-values of 0.966, 0.973, and 0.972, in the aortic valve, ascending aorta, and aortic arch, respectively (p ≤ 0.001).
The subjective image quality with regard to the diagnostic value for aortic calcification was rated lower for ultralow-dose CT images with a mean of 3.9 as compared with standard-dose images with a mean of 4.9 (p ≤ 0.001). Only one case (1%) was rated as nondiagnostic for aortic calcium detection on ultralow-dose CT.
Studies have shown a decrease in postoperative stroke rates of patients undergoing preoperative CT compared with those that don't, but it is not routinely performed prior to cardiac surgery due to the potential risk of radiation-induced malignancy. To date, standard cardiac preoperative workup includes evaluation by chest x-ray, but, as shown in the current study, this only detects large calcified areas and generally underestimates thoracic aortic atherosclerosis, the study authors noted, underlining that x-ray also lacks CT's capacity for anatomically differentiated assessment.
The study had its limitations, such as the limited number of patients included and the exclusion of patients with extensive atherosclerosis. However, there was a high agreement of calcification estimation even in patients with only minimal to moderate atherosclerosis, which, according to the authors, allowed adequate assessment of the tested technique.
They stated further studies that include patients prior to cardiac surgery may clarify the value of ultralow-dose CT as an alternative to conventional chest x-ray in a target study group and diagnostic setting, and they pointed to the CRICKET study in the Netherlands as a case in point.
"It is on us to reduce prejudice and fear of radiation dose among referring colleagues. This can be achieved by both continuous education and ongoing technical improvements that now have given us the capability of providing the accuracy of CT at the dose of a chest x-ray," Messerli noted. "Now that we can provide this tool, we may further validate the usefulness of it in different clinical scenarios and patient groups."