Automated measurement of soft plaque in the heart using coronary CT angiography (CTA) was accurate compared to the gold-standard modality, intravascular ultrasound (IVUS), and was far faster than manual methods, concluded a new report published online before print this month in Radiology.
Researchers from the University of Erlangen in Germany and from Cedars-Sinai Medical Center in Los Angeles examined a cohort of 70 patients (mean age, 55 years ± 12 for men and 58 years ± 10 for women) using two modalities, IVUS and coronary CTA, and compared the results between the two (Radiology, September 9, 2010).
The retrospective study was limited to dual-source CT datasets considered to have excellent image quality, which were compared side-by-side with corresponding IVUS data "to identify focal, noncalcified plaques in the proximal or middle section of a major coronary artery, with clearly defined proximal and distal boundaries at both CT and intravascular US," wrote study authors Damini Dey, PhD; Piotr Slomka, PhD; and Daniel Berman, MD, all from Cedars-Sinai; and Tiziano Schepis, MD; Mohamed Marwan; and Stephan Achenbach, MD, from the University of Erlangen.
The researchers aimed to test the accuracy of their previously developed automated algorithm, AUTOPLAQ (APQ), for volumetric quantification of noncalcified and calcified plaque from cardiac CT images compared to IVUS. A previous validation of the APQ technique did not include validation with IVUS.
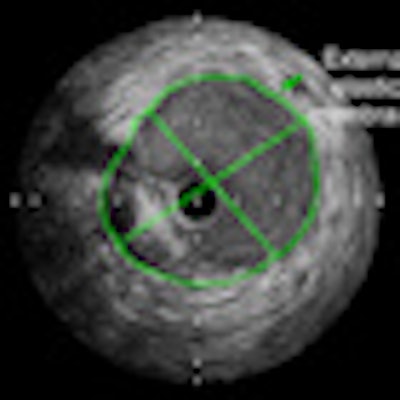
Based on American College of Cardiology (ACC) recommendations, atherosclerotic plaques were defined as those located between the media and the intima with a thickness of at least 0.5 mm, the authors wrote. Atheroma area was calculated by subtracting the luminal area from the external elastic membrane cross-sectional area. The images were analyzed by a single experienced observer.
CT scans were performed on a dual-source scanner (Somatom Definition Dual Source, Siemens Healthcare, Erlangen, Germany) following administration of oral beta-blockers to achieve a heart rate of 65 beats per minute or less, as well as 350 mg of iodinated contrast at 6 mL/sec.
Images were acquired at 120 kVp and 400 mAs per rotation using 0.6-mm collimation, with reconstructions of transaxial images at 0.75-mm section thickness, 0.4-mm increment, and a medium-soft convolution kernel (B26f).
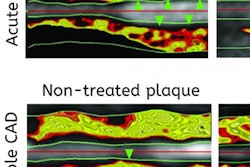
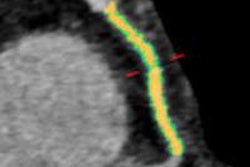
Plaque was quantified manually by an observer blinded to the IVUS results, with anatomic landmarks used to ensure that the same plaques were being evaluated. Following manual quantification, the automated APQ algorithm was applied to compute total noncalcified plaque volumes within the automatically segmented vessel boundaries, with the results displayed as color overlays on the 3D coronary CTA data for visual assessment.
The results showed excellent correlation between noncalcified plaque volumes quantified with APQ and IVUS (r = 0.94, p < 0.001). The mean noncalcified plaque volume at IVUS was 105.9 mm3 ± 83.5, compared with 116.6 mm3 ± 80.1 with the APQ software. The difference was not statistically significant (p = 0.08).
In addition, the mean noncalcified plaque volume with manual tracing from the CT images was 100.8 mm3 ± 81.7, compared with APQ at 116.6 mm3 ± 80.1, again showing excellent correlation (r = 0.92, p < 0.001) and no significant differences (p = 0.12).
In our study, there was excellent correlation, and there were no significant differences in "noncalcified plaque volumes quantified with intravascular US and multidetector CT, with both automated and manual methods," Dey and colleagues wrote.
 |
| Images show quantification of proximal left anterior descending artery plaque in a 71-year-old male nonsmoker with hypercholesterolemia. Top: Cross-sectional intravascular US view with traced external elastic membrane (green arrow) and lumen-intima border (yellow arrow). Bottom: Longitudinal intravascular US view of the plaque. Blue arrow = position of cross-sectional views. Images republished with permission of the Radiological Society of North America from Radiology, September 9, 2010, online before print, doi: 10.1148/radiol.10100681. |
Compared with manual measurements, the automated method with CTA showed a trend toward smaller absolute differences from the plaque volume quantified with IVUS, and narrower 95% limits of agreement.
At the same time, the 95% limits of agreement for IVUS and manual CT measurements were wide compared with mean plaque volumes, suggesting several possible explanations for the differences, Dey and colleagues wrote. Possible explanations include limitations in spatial and temporal resolution at CT, and the measurement of all components of the coronary vessel wall, including the adventitia, that are measured at CT.
"The adventitia was included for both manual and automated CT plaque quantification, which is a potential source of intermethod variability," the authors wrote. "Furthermore, because of these differences, measurement of outer vessel wall thickness with CT cannot be easily validated with measurement with intravascular US."
Previous studies have noted a significant overlap of CT attenuation values between lipid-rich and fibrous noncalcified plaque compared to IVUS. Nevertheless, calcified and noncalcified plaque have significantly different attenuation values, suggesting that robust differentiation is possible. Previous manual measurements have shown significant interobserver variability that is affected by plaque size and image quality.
"In our study, our patient cohort underwent intravascular US for clinical reasons, which may explain larger plaque volumes compared with those reported in recent studies," they wrote.
Among the limitations cited by the authors were the retrospective study design and relatively small sample size. They also said that future validation with atherosclerotic lesions containing both calcified and noncalcified plaque may be necessary.
The authors had previously assessed APQ's performance with atherosclerotic plaques and found that measurements of noncalcified and calcified plaque components agreed closely with measurements with manual quantification, although these results were not validated with ultrasound, the authors wrote.
"Automated scan-specific threshold level-based quantification of plaque components with coronary CT angiography allows rapid, accurate measurement of noncalcified plaque, compared with intravascular US quantification, and requires a fraction of the time needed for equivalent manual analysis," Dey and colleagues wrote.
By Eric Barnes
AuntMinnie.com staff writer
September 21, 2010
Related Reading
Advanced CT may have role in noncalcified plaque assessment, September 8, 2010
SHAPE II task force revising cardiac risk guidelines, August 17, 2010
Coronary calcium usually ignored on chest CT, August 12, 2010
Coronary calcium score doesn't help predict risk in low-risk men, June 7, 2010
CT equivalent to IVUS for culprit plaque detection, December 4, 2008
Copyright © 2010 AuntMinnie.com