VIENNA - Delegates at the 2009 European Congress of Radiology (ECR) saw a series of presentations Friday unveiling new findings and key updates on digital breast tomosynthesis (DBT). As the body of research builds in this relatively unexplored field, the advantages and limitations of DBT compared with conventional full-field digital mammography (FFDM) and other modalities are becoming better defined.
In the first of three studies comparing the clinical performance of the two technologies, Daniel Förnvik from Lund University in Sweden discussed a study that assessed their comparative performance in measuring breast cancer size.
In theory, DBT would overcome the limitations of conventional 2D FFDM, which suffers from anatomical noise created by superimposed breast structures. In the study, FFDM was performed using craniocaudal and mediolateral views while a prototype DBT system generated the 3D (DBT) data. The work was a collaborative effort with Siemens Healthcare of Erlangen, Germany.
Patients consisted of 65 women identified by FFDM as having subtle but suspicious signs of breast cancer, or who were symptomatic with subtle or negative findings on FFDM but suspicious lesions on ultrasound.
Experienced radiologists without knowledge of the pathology results measured mass sizes using DBT, FFDM, and ultrasound independently, using scatter plots and linear regression to produce predictive R2 statistics.
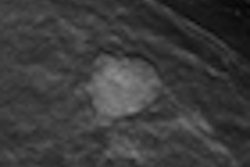
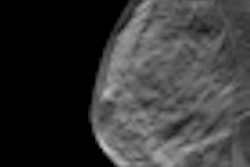
Results showed that tumor outline could be determined in significantly more cases with DBT (84%) and ultrasound (83%) than with FFDM (51%). DBT also had the highest correlation with pathology (R2 = 0.66, versus 0.49 for ultrasound and 0.47 for FFDM) and performed better when sizing smaller tumors.
"It was much easier to outline the tumor using DBT than FFDM, and [DBT] is therefore superior in the appropriate staging of breast cancer," Förnvik said. "DBT also had the highest proportion of measurable tumors, though it can be considered as complimentary to ultrasound."
Certain tumors were measurable only with DBT, and others only with ultrasound. In conclusion, Förnvik suggested that due to the increasing use of breast-conserving surgery, DBT's superior cancer sizing capability could improve diagnosis and care in the clinic.
In a major update to ongoing work, Gisella Gennaro of the Oncological Institute of Veneto in Padua, Italy, also presented her latest research on 200 patients from a blinded multireader (six radiologists) study of two-view FFDM versus one-view DBT. At ECR 2008, she presented preliminary findings on 50 patients, from three radiologists.
The expanded dataset included women with breast lesions classified by mammography and/or ultrasound as doubtful or suspicious. Six experienced radiologists reviewed left and right breasts of each patient individually, with clinical assessments from each reader compared against conclusive pathology results.
Findings were identified, localized, and rated according to the American College of Radiology's seven-step BI-RADS scale. Multiple-reader, multiple-case (MRMC) receiver operator characteristics (ROC) analysis was applied to data on a total of 371 breasts, and areas under the ROC curves across radiologists for FFDM and DBT were compared.
There was slightly lower variability with DBT than FFDM; however, it was not significant at 95% confidence intervals. Areas under the ROC curves (AUCs) for detecting breasts with malignant lesions were 0.884 with DBT versus 0.852 for FFDM. Similar results were obtained for breasts with benign lesions (0.857 for DBT versus 0.845 for FFDM).
"We found that the overall clinical performance of tomosynthesis in one view was not significantly different from FFDM in two views," Gennaro concluded. "We can say that in this study population, tomosynthesis in one view was shown to be noninferior."
The DBT prototype used was an enhancement of a standard FFDM unit (Senographe DS, GE Healthcare, Chalfont St. Giles, U.K.), modified to acquire multiple projections over a limited arc. In this case, it produced 15 projections over a 40° arc.
Gennaro commented that radiation doses delivered were in accordance with European guidelines.
In a third presentation on developments in DBT, Andrew Smith, director of imaging science at Hologic of Bedford, MA, brought fresh findings from research assessing radiologist performance variability with DBT (combined 3D + 2D data) versus FFDM (2D data alone).
In this study, 27 radiologists used BI-RADS and probability of malignancy metrics to assess 310 cases, taken from 1,000 patients. The sample consisted of normals, recalls (women recalled after screening but subsequently dismissed), women with benign lesions identified with biopsy, and 51 cancers.
Performance was measured using ROC curves and recall rates for screening cases -- variability for AUCs and recall rates were studied separately for 2D and then 2D + 3D. This analysis was performed for all images and subsets involving masses and calcifications.
The 27 readers were experienced in reading FFDM images but undertook a training course in DBT. "Superficially, these images look quite like mammograms but there is a certain expertise needed to read them efficiently," Smith noted.
Results showed that all readers improved using 2D + 3D data versus 2D alone. However, the variance (or standard deviation) under the ROC curve for 2D + 3D was 72% versus 2D alone, which was not statistically significant (p = 0.11). In a subgroup with calcifications, there was no significant improvement in 2D + 3D versus 2D alone.
In a group without calcifications -- but where lesions and architectural distortions were present -- variance for 2D + 3D was statistically significant at 62% (p = 0.02).
On decisions to recall in noncancer cases, Smith found that 71% of radiologists were in agreement using 2D (FFDM) alone, compared with 79% using 2D + 3D data. Therefore, there was a statistically significant difference in radiologists agreeing what was "normal."
"Radiologists are more accurate, as measured by area under the curve, and more confident, as measured by variance, using 2D + 3D versus 2D alone," Smith said. "The main goal is precancer detection and this [2D + 3D] shows great potential. It's certainly conceivable and likely that 3D imaging [DBT] will become the standard of care long term."
By Rob Skelding
AuntMinnie.com contributing writer
March 7, 2009
Related Reading
New breast imaging applications show diagnostic promise, January 20, 2009
Pilot study: DBT's role needs further research, April 18, 2008
ECR sessions examine DBT's effectiveness, March 7, 2008
Copyright © 2009 AuntMinnie.com