A breast computer-aided detection (CAD) system can be deployed to improve screening efficacy by independently identifying suspicious nonreferred cases, Dutch researchers have found. A team led by Dr. Jaime Melendez from the Diagnostic Image Analysis Group at Radboud University Nijmegen Medical Center found a standalone CAD system could have detected more than 10% of breast cancer cases that had been missed at double reading.
"Using a CAD system that autonomously detects potentially missed cancers could substantially improve screening efficacy with only a small additional reading effort," he noted.
Screening mammography exams can be difficult to assess, and a substantial percentage of screening-detected cancers can be seen in retrospect on prior mammograms. Widely used in screening today, CAD is effective for detecting microcalcifications. Its utility with masses is more controversial, however, as many radiologists consider it not to be useful due to specificity issues, Melendez said. He explained that CAD is currently utilized to reduce perception errors and is not intended to improve decision-making.
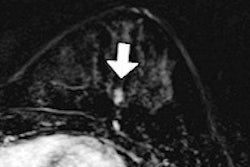
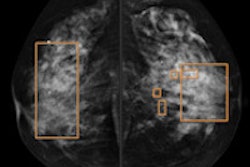
 Subtle mass that was not recalled during screening, but detected on CAD. Top row: Exams that were not recalled during screening. Bottom row: Exams where lesion was detected in a later screening round. All images courtesy of Dr. Jaime Melendez.
Subtle mass that was not recalled during screening, but detected on CAD. Top row: Exams that were not recalled during screening. Bottom row: Exams where lesion was detected in a later screening round. All images courtesy of Dr. Jaime Melendez.
The Radboud team sought to investigate the use of CAD after initial double reading had been performed. In this approach, a standalone CAD system would select the most suspicious cases that were not recalled, and these cases would be reconsidered by an arbiter.
They also wanted to evaluate different techniques for pattern recognition techniques for a highly specific operating point (2% recall rate).
Focusing on the detection of masses and architectural distortions, the research group selected 9,393 cases (28,811 scanned film images) from the Dutch screening program's large heterogeneous database. Of the 9,393 cases, 266 were abnormal cases with priors showing visible masses and architectural distortions that were not detected after double reading. The remaining 9,127 randomly selected normal cases showed no sign of pathology during follow-up.
"In this particular study, we have investigated some basic and state-of-the-art pattern recognition techniques and optimized their parameters using a large and heterogeneous database consisting of prior exams with visible masses and architectural distortions, and a large number of normal cases, which follows the distribution observed in screening settings," Melendez told AuntMinnieEurope.com. "The application mode of our CAD system would be to run it on the set of not-recalled cases in order to generate an additional set with the most suspicious exemplars, and then send these exemplars to a third radiologist for reconsideration, assuming that double reading is already practiced, as is generally the case in Europe."
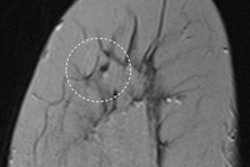
 Architectural distortion that was not recalled during screening, but detected on CAD. Top row: Exams that were not recalled during screening: Bottom row: Exams where lesion was detected in a later screening round.
Architectural distortion that was not recalled during screening, but detected on CAD. Top row: Exams that were not recalled during screening: Bottom row: Exams where lesion was detected in a later screening round.
Three different region classifier techniques: Linear Discriminant Classifier (LDC), GentleBoost with Regression Stumps (GB-RS), and Support Vector Machine with Radial Basis Function Kernel (SVM-RBF) were evaluated on the cases.
Mean case sensitivity by classifier technique at 2% recall rate
- SVM-RBF: 10.5%
- GB-RS: 9.8%
- LDC: 4%
"Detection of early signs of malignancy by means of a standalone CAD system is feasible at low recall rates," Melendez said. He presented the findings at the RSNA 2012 meeting in Chicago.
He noted one of the system's advantages is it can be run offline, although a human arbiter is still needed to make the final decision on the case.
"This arbiter could also contribute to increase the specificity of the system, thus reducing the number of unnecessary recalls," he said.