A new study by Belgian researchers indicates that digital tomosynthesis could be useful for assessing ureteral and kidney stones, particularly for screening patients prior to CT. But the digital radiography technique has different levels of accuracy depending on the location and size of stones.
Conventional radiography (both analog and digital) has low sensitivity and specificity in detecting nephroureterolithiasis. CT is much better but it involves a higher radiation dose, especially for patients undergoing extracorporeal shockwave lithotripsy, who sometimes get repeat CT scans to track stone migration and fragmentation, according to a satellite symposium at last month's European Congress of Radiology (ECR) by Dr. Koen Mermuys from AZ St.-Jan Hospital in Brugge, Belgium.
Could digital tomosynthesis offer an acceptable alternative? Digital tomo units are based on a panning tube head that moves in an arc around the patient, which could help radiologists see around superimposed anatomy that can obscure stones on conventional radiography, Mermuys said.
The group set up a clinical study that compared the diagnostic value of digital tomosynthesis and standard radiography, using CT as the gold standard. In addition to assessing sensitivity and specificity of the three modalities for both kidney and ureteral stones, the group also measured radiation dose.
Over seven months ending October 2008, the group accrued 50 patients, with an average age of 51. All patients were presenting for CT to rule out nephroureterolithiasis, and they received additional anteroposterior (AP) and lateral conventional radiography, as well as digital tomosynthesis exams. Images were read by two blinded readers.
The group used both high-dose (120 kV, 280 mAs) and low-dose CT (100 kV, 140 mAs) protocols. The tomosynthesis protocol acquired 78 slices per study in the AP view (VolumeRad option for Definium 8000, GE Healthcare, Chalfont St. Giles, U.K.), at a slice interval of 3 mm. The readers reviewed the images by scrolling through the slices on a workstation.
The researchers analyzed the data in two ways, first by determining whether the patient had stones, then on a per-stone analysis. The per-stone analysis was further subdivided by stone location (kidney or ureter) and stone size (smaller than 2 mm, 2-5 mm, and larger than 5 mm).
Of the 50 patients, 31 had a total of 78 stones. Of these, 64 were in the kidney, 18 were smaller than 2 mm, 33 were 2-5 mm, and 13 were larger than 5 mm. There were 14 ureteral stones.
Not surprisingly, conventional radiography turned in less-than-impressive numbers. For both kidney and ureteral stones and on a per-stone basis, the conventional technique had a sensitivity of 23%; broken down by stone type, sensitivity was 22% for kidney stones and 28% for ureteral stones. Tomosynthesis, on the other hand, reported sensitivity of 56% for both types of stones and 61% for kidney stones alone. Digital tomo's sensitivity for ureteral stones was a disappointing 32%.
 |
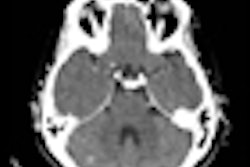
| Two lithiasis in left kidney, seen on both techniques but much clearer on the tomosynthesis image (above), as well as nice visualization of the contour of the kidney. Images courtesy of Dr. Koen Mermuys. |
 |
Although digital tomo's sensitivity nearly tripled for both types of stones compared to conventional radiography, 61% sensitivity is nothing to write home about. The group further analyzed the data to determine what was affecting the modality's performance -- and found that stone size was the main culprit.
For stones smaller than 2 mm, conventional radiography had sensitivity of 5% and tomosynthesis turned in 20%. However, when only stones larger than 2 mm were included in the analysis, digital tomosynthesis produced sensitivity in the range of 75% for the 2-5 mm subgroup and 85% for those larger than 5 mm. This compared to 24% for stones 2-5 mm in size and 39% for stones larger than 5 mm with conventional radiography.
"With the increasing size of stones, the sensitivity rises for both radiography and tomosynthesis, but for tomo the increase is much higher," Mermuys said. "For the small stones, they're just too small, and then we have trouble with noise versus microlithiasis."
Tomo also performed poorly for ureteral stones, which Mermuys attributed to the lack of visualization of the urethral wall. In kidney images, there is nice delineation of the contour of the organ, which makes it easier to interpret. A larger study sample size for ureteral stones might produce a statistically significant improvement in sensitivity, he said.
In the radiation dose analysis, the group found that tomosynthesis produced a radiation dose of 0.85 mSv, an increase of 70% compared to 0.5 mSv for radiography. Tomo produced a dose savings of 66% compared to low-dose CT (2.5 mSv) and 93% compared to high-dose CT (12.6 mSv).
Mermuys concluded by saying that digital tomosynthesis shouldn't be considered a replacement for CT, but it could play a role in primary screening of patients who present to the emergency room with suspicion of renal colic. Using the technique in combination with ultrasound could improve accuracy even further, he said.
"Probably a lot of these patients won't end up in CT because you will have seen whether they have stones with the combination of tomosynthesis and ultrasound," Mermuys said.
By Brian Casey
AuntMinnie.com staff writer
April 2, 2009
Related Reading
Italian study backs tomosynthesis over DR for lung pathology, February 18, 2009
Digital chest tomo beats standard DR for pulmonary nodules, October 21, 2008
Digital tomosynthesis beats standard DR in finding chest lesions, August 11, 2008
TMJ imaging benefits from digital tomo technique, December 24, 2007
DR pumps new life into tomosynthesis-based radiography, October 29, 2007
Copyright © 2009 AuntMinnie.com