Patients with positive findings on both coronary CT angiography (CCTA) and SPECT myocardial perfusion imaging (MPI) are at high risk of cardiac events, while negative results on both exams confer an excellent long-term prognosis, according to a study presented at last week's European Society of Cardiology congress (ESC).
Investigators from University Hospital Zurich in Switzerland examined almost 400 patients who underwent clinically indicated SPECT and CCTA, following them for almost seven years on average to assess for cardiac events. Matched positive findings in both modalities conferred high risk, while matched negative findings in both led to very low event rates, with unmatched findings falling in between the two.
Powerful combination
 Dr. Aju Pazhenkottil from University Hospital Zurich.
Dr. Aju Pazhenkottil from University Hospital Zurich."The conclusion is that there is a long-term prognostic value of hybrid imaging, and that the matched finding is actually associated with worse outcome," said cardiologist and lead author Dr. Aju Pazhenkottil in an interview with AuntMinnieEurope.com. "If both studies were normal, then these patients had a really good prognosis."
Cardiac hybrid imaging combining SPECT MPI with CCTA offers information on both coronary anatomy and myocardial perfusion for diagnosing coronary artery disease. But, the authors noted in an abstract, studies on the prognostic value of the hybrid diagnostic combination are scarce. Therefore, the study assessed the long-term value of cardiac hybrid imaging with the two modalities.
3 categories, 2 tests
In all, 428 patients were examined with both modalities and classified into three groups based on their hybrid cardiac imaging findings, including the following:
- Stenosis by CCTA and matching reversible SPECT defect
- Unmatched CCTA and SPECT finding
- Normal findings by both CCTA and SPECT
The study end points were all-cause death or nonfatal myocardial infarction (MI), deemed hard events, and also a composite of major adverse cardiac events (MACE) that included death, MI, unstable angina requiring hospitalization, and coronary revascularizations.
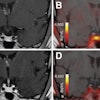
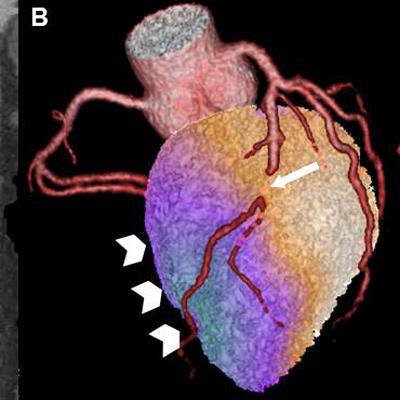
 Cardiac hybrid image showing a matched hybrid finding with a stenosis in the LAD (arrow: A = multiplanar reconstruction of a CT coronary angiography) causing a perfusion defect at stress (arrowhead: B), which is reversible at rest (C). All images courtesy of Dr. Aju Pazhenkottil.
Cardiac hybrid image showing a matched hybrid finding with a stenosis in the LAD (arrow: A = multiplanar reconstruction of a CT coronary angiography) causing a perfusion defect at stress (arrowhead: B), which is reversible at rest (C). All images courtesy of Dr. Aju Pazhenkottil.The researchers used the Kaplan-Meier estimate to determine survival free of MACE. They applied Cox's proportional hazard regression to determine independent predictors for cardiac events.
"MACE is myocardial infarction and unstable angina requiring hospitalization as well as coronary resvascularization, so it's a combined end point," Pazhenkottil explained.
One-third had events
Among the 428 patients, 14 were lost to follow-up and 39 were excluded due to revascularization within 30 days of the start of the study, leaving 375 patients for analysis. During a median follow-up of 6.8 years, there were 160 major adverse cardiac events in 109 patients, representing 29% of the population, including 45 deaths (12%) and 19 nonfatal myocardial infarctions, the group reported.
 Above: Cardiac hybrid findings predict cumulative incidence rate of MACE (death, myocardial infarction, unstable angina requiring hospitalization and coronary revascularization). Below: Hybrid findings predict hard events including death and myocardial infarction.
Above: Cardiac hybrid findings predict cumulative incidence rate of MACE (death, myocardial infarction, unstable angina requiring hospitalization and coronary revascularization). Below: Hybrid findings predict hard events including death and myocardial infarction.There were 78 late revascularizations, including 63 percutaneous coronary interventions and 15 coronary artery bypass grafts.
Normal findings in both modalities were found in 216 patients (58%), and a matched defect was found in 46 patients (12%), with unmatched findings in 113 patients (58%), according to the researchers.
Patients with matched findings had the highest rate of hard events annually at 7%. Unmatched findings led to a lower event rate, and events were lowest in those with matched negative findings, the group reported. MACE rates followed a similar pattern.
| Patient results | Hard events | MACE | p-value |
| Matched positive | 7.0% | 21.8% | |
| Unmatched findings | 3.7% | 9.0% | |
| Matched negative | 1.2% | 2.4% | (p < 0.01 for all) |
Corresponding matched hybrid image findings were an independent predictor for MACE. However, they were not an independent predictor of hard events, the researchers noted.
Set diagnostic algorithm for today
The procedure is now well-established for the use of hybrid imaging, Pazhenkottil said.
"What we do is usually the CCTA first with low to intermediate probability of disease, and if CT is completely normal or 20% to 30% stenosis -- below 50% -- then we don't do SPECT at all," he said. "If there's a stenosis above 50%, we go on with the stress MPI [treadmill test] and if stress MPI is normal, the radiation dose can be even lower, so we don't do SPECT if the stress test is normal."
Patients with normal findings on hybrid imaging had an excellent event-free survival. It wasn't the first time the study team had come to this conclusion, but it was the largest study population and duration to date, Pazhenkottil told AuntMinnieEurope.com.
"We looked at these kinds of patients in 2011 in the European Heart Journal, but with a shorter follow-up period -- around 300 patients," he said. "And we had almost the same conclusion."
But this time it's 400 patients and a seven-year follow-up -- "really up to 10 years, so it's been established now and in other cardiac centers," Pazhenkottil added.
The patients weren't signed up for both exams from the start, he cautioned, but both were clinically indicated, and the study looked at patients who happened to have both, a common occurrence to clarify the results.
For example, "maybe they didn't look at the CT before, or sometimes they looked at it and the stenosis was 50%, and we didn't know if it was causing ischemia or not -- so that's why we did both of the tests," he said.
SPECT is one of the most established tests available for diagnosing coronary disease, so it makes a good pairing with CT, Pazhenkottil said, adding that there are several other good options on the horizon.
But other combinations coming
"It's not yet established, but I believe there might be good functional tests with CT alone; there are some ongoing studies with CT perfusion, looking at contrast and perfusion as well," he said. "And now you can do CT and calculated fractional flow reserve."
Finally, there are studies looking at transluminal attenuation gradients and contrast opacification that look at the contrast medium before and after the stenosis. PET and MR might cost a little more but are also promising.
In fact, any of these might turn into a good substitute for CT plus SPECT, but the evidence for this particular combination is strong, he said.