An institution in Spain has adopted single reading with computer-aided detection (CAD) software to screen for breast cancer in light of recent study results indicating that it works just as well as double reading with arbitration. The only caveat is the readers must be experienced radiologists.
Screening mammography is an imperfect process, with sensitivity estimated at about 70% to 85%. As such, double reading with arbitration is the standard protocol in Europe, because it increases cancer detection rates by 5% to 15%. In most double-reading protocols, an experienced breast radiologist is usually paired with a general diagnostic radiologist or even a radiographer; single reading is allowed once a radiologist's performance has been assessed.
The latter provision raises the question of whether double reading could be replaced entirely by a single reader, with CAD as a backup. Lead author Dr. Xavier Bargalló from the radiology department at the Hospital Clínic de Barcelona and colleagues led a team of researchers who sought to answer this question (European Journal of Radiology, 13 August 2014).
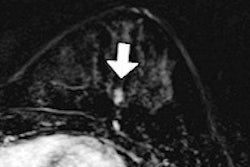
 A 62-year-old woman with invasive ductal carcinoma 11 mm in size. Above: Plain digital mammography with a focal asymmetry in left breast. Below: CAD correctly detected the lesion. All images courtesy of Dr. Xavier Bargalló.
A 62-year-old woman with invasive ductal carcinoma 11 mm in size. Above: Plain digital mammography with a focal asymmetry in left breast. Below: CAD correctly detected the lesion. All images courtesy of Dr. Xavier Bargalló.Prospective study
The prospective study included data from 21,321 consecutive screening mammograms (Senographe 2000D, GE Healthcare) in incident rounds (2010-2012). Exams were interpreted in a protocol that included single reading plus CAD (SecondLook, Premier, iCAD). These studies were then compared with data from 47,462 consecutive screening mammograms in incident rounds (2004-2010) that were interpreted following a protocol with double reading plus arbitration.
For the single reading, radiologists were selected based on their previous performance, according to the authors. They read the mammograms and made a decision whether to recall the patient, at which point the CAD marks were engaged. The radiologists then revised the marks and made a final decision.
If the final decision was that the mammographic findings were BI-RADS 1 or 2, CAD marks were not considered. If the finding was considered to be BI-RADS 0, 4, or 5, the patient was recalled and the radiologist wrote down the type of recall:
- Type A: The radiologist had found a mammographic finding that CAD did not mark.
- Type B: The radiologist had found a mammographic finding that CAD also marked.
- Type C: The radiologist found the mammogram to be BI-RADS 1 or 2 but after considering the CAD marks, determined a lesion could be present and decided to recall, meaning CAD changed the radiologist's mind.
| Mammography interpretation by reading protocol | ||||
| Cancer detection rate | Recall rate | Positive predictive value of recall | Average size of invasive cancers | |
| Single reading plus CAD | 6.1% | 7.02% | 8.69% | 14.7 ± 9.5 mm |
| Double reading | 5.25% | 7.24% | 13.32% | 14.3 ± 9.5 mm |
The increase in the cancer detection rate, which was 16.2% for double reading, wasn't statistically significant, but it can be considered relevant because it implies that up to 40 more cancers could have been detected in the historical period if the new reading system had been used, according to the researchers.
"On the other hand, that increase in detection was not directly attributable to CAD, because none of the readers recognized that CAD prompted a cancer not previously perceived by the radiologist," they wrote. "Thus, we recorded 25 type C recalls and none of them turned out to be cancer. Therefore, we think that the improvement in the performance of the program might be mainly related to the improvement in the readers."
Specialized breast radiologists performed better than general radiologists. Also, CAD did not detect any cancer not perceived previously by the radiologist, according to the authors.
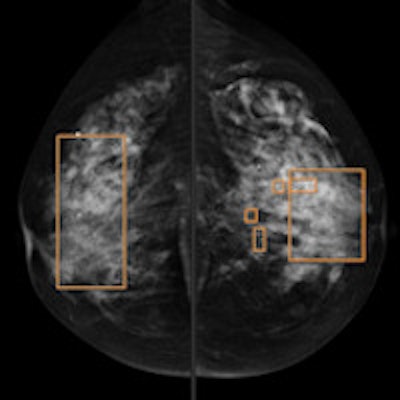
 A 57-year-old woman with invasive ductal carcinoma 18 mm in size. CAD rectangles indicate calcifications. In the upper outer quadrant of the left breast, an architectural distortion not detected by CAD can be seen.
A 57-year-old woman with invasive ductal carcinoma 18 mm in size. CAD rectangles indicate calcifications. In the upper outer quadrant of the left breast, an architectural distortion not detected by CAD can be seen.Now standard protocol
The protocol of single reading plus CAD is now standard operating procedure at Hospital Clínic de Barcelona.
"In view of the results of our study, we have adopted this protocol as a standard practice in our institution," Bargalló wrote in an email to AuntMinnieEurope.com.
 A 58-year-old woman with in-situ ductal carcinoma 29 mm in size. Immunohistochemical staining demonstrated focus of microinfiltration (1 mm). In digital mammography, some pleomorphic calcifications correctly depicted by CAD can be seen.
A 58-year-old woman with in-situ ductal carcinoma 29 mm in size. Immunohistochemical staining demonstrated focus of microinfiltration (1 mm). In digital mammography, some pleomorphic calcifications correctly depicted by CAD can be seen.Other institutions could adopt the practice as well, provided they have historical annual audits to be able to know which readers could be selected to read with CAD. "The appropriate selection of radiologists is vital in order to reach a good cancer detection rate," he added.
In his email, Bargalló emphasized that experienced readers are more confident in their own judgment; therefore, some dismissed CAD marks could actually correspond to cancers.
"On the other hand, it is well known that some CAD marks are, in retrospect, cancers but the point is that many of these marks are not actionable in a standard clinical setting, [and] CAD could actually influence [the reader] in a subtle way," he wrote.
Because the protocol has been definitely implemented as a clinical practice in his institution, Bargalló and his colleagues will keep observing their results with the intention of lowering their recall rates, he stated. And if a new version of the software becomes available in the future, it could be included in a new research study.