VIENNA - The overwhelming thirst for basic knowledge was evident at Thursday's Mini Course on skeletal radiology, as delegates crammed into Room E2 to hear insights from Dr. Iain McCall, former European Society of Radiology (ESR) president and a gold medalist at ECR 2012.
McCall was keen to highlight how radiologists must approach the analysis and interpretation of plain film radiographs in a structured format. Vital to building up an understanding of plain film was recognizing the features of differing responses of the bone, joints, and soft tissue to various disease processes and trauma, he explained.
The availability and relative cheapness of plain film make it the first-line investigation in the
 Dr. Iain McCall from Oswestry, U.K.
Dr. Iain McCall from Oswestry, U.K."As you all know, orthopedic surgeons love quantification. They'll draw a line or an angle on almost every radiograph they have," said McCall, formerly a professor of radiological sciences at the University of Keele and consultant MSK radiologist at Oswestry's Orthopaedic Hospital in the U.K.
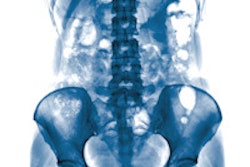
He pointed to several standard views of the lumbar spine in which quantification of the acetabular index had been conducted for congenital diaphragmatic hernia. While in these images dislocation was clearly visible, in some circumstances dislocation is less well-defined, and in those cases quantification is of key assistance to the diagnostic process.
Continuing his talk in the structured manner he favors for the interpretation of plain film, McCall's first key point was to always have two views.
"Never settle for one view. Fundamental fact: If you take nothing else from this lecture, make absolutely sure that you have two views at least," he insisted.
He demonstrated this by showing delegates images of a limb in which there was a sclerotic focus on the bone shaft in the anteroposterior (AP) view. Radiologists might be torn between a diagnosis of a calcified disk or a superimposed lymph node. The lateral view, however, showed cortical thickening, and further investigation with CT revealed benign cortical thickening in the anterior aspect of the tibia.
His second take-home message was to know normal anatomy and its appearances -- as well as its variants.
"If you do not know what the plain film looks like normally, then it is very difficult to make a diagnosis of an abnormality," said McCall, pointing to images of a normal wrist in AP, oblique, and lateral views all giving different information about the relationships of the carpal bones. "Any examination of junior trainee radiologists should include a test of their knowledge of normal anatomy."
Radiologists should also remember the numerous normal variants, as demonstrated by a view of the normal lumbar spine and one of a limbus vertebra -- a variant of the normal growth process, according to McCall. "There are some very well-established textbooks which guide you, and you should always have them nearby when you are reporting so that you can refer to them," he said.
Originally published in ECR Today on 7 March 2014.
Copyright © 2014 European Society of Radiology