Brain stones -- large solid intracranial calcifications -- are more common than previously thought, and while MRI sequences like gradient echo T2* and susceptibility-weighted imaging can be useful adjuncts, CT is now the mainstay in identifying and characterizing these intriguing items, Belgian researchers have asserted.
"The challenge of reaching a radiological diagnosis on the basis of their presence has remained an intellectual curiosity," pointed out Dr. Froilan Celzo and colleagues from the department of radiology at Antwerp University Hospital in Edegem. "Imaging findings combined with essential clinical information can help in narrowing the differential diagnosis, determining disease state, or evaluating effect of therapy."


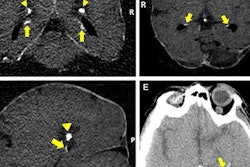
 A 60-year-old man known to have HIV presented with seizures. The solid calcifications on noncontrast enhanced CT (NCECT) at the right frontal (left), left basal ganglia (middle), and right parietal areas (right) represent sequela following treatment for documented toxoplasmosis. All images courtesy of Dr. Froilan Celzo.
A 60-year-old man known to have HIV presented with seizures. The solid calcifications on noncontrast enhanced CT (NCECT) at the right frontal (left), left basal ganglia (middle), and right parietal areas (right) represent sequela following treatment for documented toxoplasmosis. All images courtesy of Dr. Froilan Celzo.
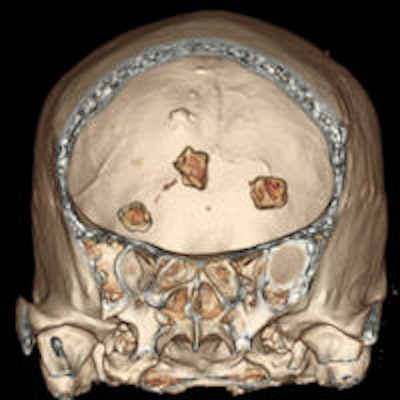
 Same patient: Coronal (left) and sagittal (right) 3D reconstructions are shown.
Same patient: Coronal (left) and sagittal (right) 3D reconstructions are shown.Also known as cerebral calculi, brain stones may be extra- or intra-axial in location. Extra-axial brain stones comprise tumors and exaggerated physiological calcifications, while intra-axial calcifications can be classified under neoplastic, vascular, infectious, congenital, and endocrine/metabolic etiologies, they wrotein an article published online on 11 September by Insights into Imaging.
"These lesions were once thought to be rare and were mostly seen in patients with seizures. Intracerebral hematomas, tuberculomas, and brain abscesses were postulated to be the most common underlying pathologies leading to the development of these intracranial calcifications," the authors noted.
The superiority of CT over x-ray in detecting macroscopic intracranial calcifications has resulted in routine visualization of various forms and sizes of brain stones. Despite the ability of CT to quantify calcification, the subjective designation of intracranial calcifications as brain stones has been considered of less importance lately, they added.
Because of its multiplanar reconstruction and 3D reconstruction capabilities, CT has supplanted the use of skull x-rays in the diagnosis of intracranial pathology. Also, CT is better than MRI in identifying and characterizing intracranial calcification, although newer MRI sequences are promising. In certain clinical situations, neurological symptoms correlate better with MRI findings than with the corresponding CT-identified calcifications.
"Various imaging findings have been found to suggest an extra-axial localization of brain lesions such as buckling of adjacent white matter, expansion of the ipsilateral subarachnoid space, presence of bony reactions and the 'dural tail' sign," Celzo et al noted. "The most common extra-axial etiologies of brain stones include meningiomas, dural osteomas, calcifying tumors (e.g. craniopharyngiomas) as well as exaggerated physiological calcifications."
Macroscopic calcifications are present in meningiomas in up to 60% of cases, the pattern of which may range from diffuse, rim, or sand-like to focal or even globular. Calcified meningiomas can be associated with focal thickening of the overlying skull bones or with dilatation of the adjacent air-containing sinus of the skull base, they stated.
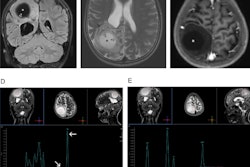
Central nervous system infections, leading to intracranial calcification, are most often seen in congenital childhood infections, particularly the "TORCH" group, which includes toxoplasmosis, rubella, cytomegalovirus, and herpes simplex infections.
As with vascular pathologies, the mechanism of calcification involved in these infections is dystrophic calcification, according to the authors. With congenital toxoplasmosis and cytomegalovirus infections, these calcifications are usually seen in the basal ganglia and periventricular areas, whereas with herpes simplex infections, the calcifications are located in the thalamic, periventricular, and gyral regions.
The dense calcifications seen in patients with congenital toxoplasmosis can also have a random distribution, with lesion sizes that correlate with the duration of infection. Treatment can result in shrinkage and even resolution of these calcifications (see figure).
Congenital rubella infections usually result in calcifications in the basal ganglia, periventricular regions, and brainstem, they noted. Congenital herpes infection can lead to chronic encephalitis resulting in extensive encephalomalacia and coarse calcification in the remaining brain parenchyma.
Granulomatous infections such as tuberculosis as well as parasitic infections such as neurocysticercosis and cerebral hydatid cyst disease can also result in characteristic intracranial calcifications.
"Knowledge of a history of travel to endemic areas together with biochemical tests, clinical data, and specific imaging findings can often lead to a confident diagnosis," Celzo and colleagues wrote. "Tuberculosis can result in intracranial calcification in 10-20% of cases and is usually located supratentorially in adults and infratentorially in children. Calcified tuberculomas can range in size from about a centimeter to several centimeters and can appear as a 'broken shell' or a dense centrally located lobulated calcification."
Neurocysticercosis is the leading cause of adult-onset seizures in less developed countries, as shown by epidemiological studies, with no consensus on whether the intracranial calcifications are epileptogenic or not, they added. The calcifications represent dead larvae and appear as a dense calcified cyst that sometimes contains a dense eccentric nodule. Lastly, cerebral hydatid disease is an extremely rare cause of intracranial calcification. The lesions are usually single, septated, or multilocular and represent the dead parasite, the authors concluded.