Far from being a deterrent to evaluating plaque composition using CT, the use of iterative reconstruction has no effect on the visualization of plaque type, and improves image quality overall while reducing dose, according to Dutch research presented at last month's RSNA meeting in Chicago.
The group's analysis of 55 coronary arteries in the study showed noise was reduced by nearly half with the use of iterative reconstruction, while signal-to-noise ratio and contrast-to-noise ratios each improved by about 75%. Importantly, iterative reconstruction had no effect on measurements of plaque volume or cross-sectional luminal area, the researchers reported.
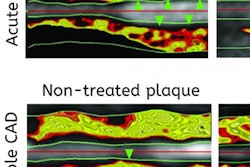
Data from the recent CONFIRM registry suggest noncalcified plaques are independent predictors of future cardiovascular events over calcified plaques alone. "So detection and quantification of these plaques may allow for more effective risk stratification," said Dr. Richard Takx from University Medical Center Utrecht in his presentation.
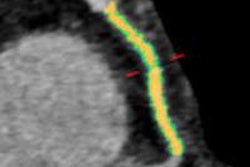
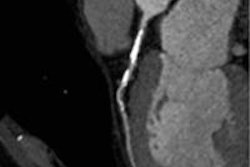
 A 54-year-old man with a body mass index of 26.9 underwent coronary CT angiography using a step-and-shoot protocol (140 mAs, 225 mAs, DLP 342.3). In images reconstructed using FBP (left) and various levels of iterative reconstruction (IR) with iDOSE 4 (Philips Healthcare), noise reductions can seen in the IR images (right), but attenuation and plaque volumes are essentially unchanged. Images courtesy of Dr. Richard Takx.
A 54-year-old man with a body mass index of 26.9 underwent coronary CT angiography using a step-and-shoot protocol (140 mAs, 225 mAs, DLP 342.3). In images reconstructed using FBP (left) and various levels of iterative reconstruction (IR) with iDOSE 4 (Philips Healthcare), noise reductions can seen in the IR images (right), but attenuation and plaque volumes are essentially unchanged. Images courtesy of Dr. Richard Takx.But while iterative reconstruction is implemented more and more in practice, there are little data assessing the effect of different levels of iterative reconstruction on the detection and characterization of noncalcified plaques, he said.
"The aim of this study was to compare coronary plaque size and composition as well as the degree of coronary artery stenosis on CCTA [coronary CT angiography] using three different levels of iterative reconstruction [IR] and filtered back projection [FBP]," he said.
The study team analyzed 63 patients (45 men, 18 women, mean age 50.8 ± 13.0 years) who underwent CCTA using a step-and-shoot protocol on a 256-detector-row scanner (Brilliance iCT, Philips Healthcare). Takx and colleagues Dr. Martin Willemink, Dr. Arnold Schilham et al reconstructed the raw CT data using FBP and three different levels (2, 4, 6) of the IR reconstruction algorithm (iDOSE 4, Philips Healthcare).
They calculated CT attenuation and noise in the aorta and two coronary arteries, and also calculated signal-to-noise-ratio (SNR) and contrast- to-noise-ratio (CNR). Finally, they measured volumes of lipids (-10 to -69 HU). Lesion boundaries for volume measurement of the different plaque types were manually set immediately above and below the defined thresholds for the three plaque types.
As for statistical analysis, RM-ANOVA was used to determine statistical significance in the means across the different reconstructions. To correct for multiple tests, a Bonferroni adjustment was applied for posthoc analysis.
The results showed IR had no effect on measurements of plaque volumes:
| Plaque component and luminal area measurements using various reconstructions | |||||
| FBP | IR 2 | IR 4 | IR 6 | P value | |
| Lipid mm3 | 4.1 ± 11.0 | 2.9 ± 7.4 | 3.5 ± 9.3 | 3.3 ± 9.4 | 0.071 |
| Fibrous mm3 | 5.9 ± 11.2 | 4.8 ± 7.5 | 5.4 ± 9.4 | 5.2 ± 10.1 | 0.275 |
| Calcified mm3 | 43.3 ± 50.6 | 42.2 ± 48.5 | 42.7 ± 50.3 | 41.5 ± 48.2 | 0.415 |
| Luminal area mm2 | 13.6 ± 4.7 | 13.6 ± 4.6 | 13.6 ± 4.6 | 13.5 ± 4.6 | 0.613 |
| Luminal area mm2 | 13.6 ± 4.7 | 13.6 ± 4.6 | 13.6 ± 4.6 | 13.5 ± 4.6 | 0.613 |
However, image quality improved dramatically, mostly owing to noise reduction. Image noise fell by 42% (p < 0.0001), while SNR in the aorta rose by 72.5% (p < 0.001) and CNR by 72.0% when iterative reconstruction was dialed up to level 6, for example.
Of the two vessels studied, IR improved noise more in the aorta (by 28.2%) than in the left main artery (13.8%) and the right coronary artery (all p < 0.0001), Takx said.
"CT attenuation and didn't differ that much, but in the left main artery there was a significant difference between FBP and IR 6," he said. There was also a significant difference in attenuation in the right coronary artery based on the reconstruction method, "but the amount was quite small so we don't think it's clinically relevant or significant," he added.
The mean cross-sectional area (13.6 ± 4.7 mm2 at FBP and 13.5 ± 4.6 mm2 at IR level 6, p = 0.613) also didn't differ significantly based on reconstruction method.
Likewise, plaque volumes (53.0 ± 63.9 mm3 at FBP and 50.1 ± 60.0 mm3 at IR level 6), did not vary significantly based on reconstruction method. And application of IR did not lead to significant differences in plaque component volumes, Takx said.
"What we do see is a significant decrease in image noise, [and] an increase in contrast-to-noise ratios, which are greatest in the aorta and least in the right main and left coronary arteries," he said.
Compared with FPB application of iDose on CCTA exams, iterative reconstruction in CCTA images improved quantitative image quality parameters while allowing for the reliable assessment of plaque composition and cross-sectional luminal areas, Takx said. "So in the future you can use iterative reconstruction with iDOSE," he said.
The study was published online ahead of print in the International Journal of Cardiovascular Imaging (19 September 2013).