The stunning success of cardiac CT perfusion has led some experts to question whether nuclear cardiology has a future, but it may be premature to write off nuclear cardiology. It is a robust, tried, and tested field supported by very established data, according to Dr. Ashley Groves, a radiologist and nuclear medicine physician at the Institute of Nuclear Medicine (INM) at University College Hospital in London.
"Nuclear coronary angiography must not be thought of in terms of competing technology but complementary technology. The vision of a single noninvasive cardiac test has finally arrived. The future for cardiac CT perfusion looks promising, but we're not there yet," he told delegates at the recent British Institute of Radiology (BIR) President's Conference in London.
Groves is a part of a multidisciplinary team in one of the largest and busiest single-site nuclear medicine departments in the U.K. Together, the team of scientists -- physicists, doctors, chemists, pharmacists, specialist technicians, radiographers, and nurses, as well as administrative support staff -- form the backbone of the INM.
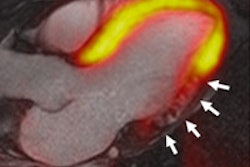
 Rubidium PET myocardial perfusion study shows that even during cardiac stress, there is no inducible ischemia. Images courtesy of Dr. Ashley Groves.
Rubidium PET myocardial perfusion study shows that even during cardiac stress, there is no inducible ischemia. Images courtesy of Dr. Ashley Groves.Between them, the clinical service currently undertakes nearly 15,000 studies per annum, including more than 4,000 PET/CT studies and more than 100 radionuclide therapy administrations. The INM's installed base includes two PET/CT systems (a 16-slice system and a 64-slice system), two SPET/CT systems, two further SPET gamma camera systems, a solid-state dedicated cardiac camera (D-SPECT), a dual-energy x-ray absorptiometry (DEXA) system, and a full range of supporting nuclear medicine instrumentation. The center performs a wide range of routine and experimental in- and out-patient radionuclide therapy procedures inclusive of radioiodine, strontium, lutetium, and metaiodobenzylguanidine (MIBG).
"There have been multiple developments in hardware with solid-state detector PET/CT, which has improved sensitivity and specificity. Also in software, gated acquisitions and the capability to produce iterative reconstructions is now routinely provided," he explained.
Ultimately, physicians have better performing equipment and patients have less radiation exposure, which means that myocardial perfusion is becoming a reality in routine practice, Groves added. Diagnostic performance with D-SPECT is good, but in populations with a large number of normal patients, specificity can be limited. He cautioned that "the Achilles heel of the technique" -- the so-called "triple vessel disease" -- also means nuclear technology remains poor at diagnosing this type of disease.
Meta-analysis studies have shown 87% sensitivity and 73% specificity, which is good but not as perfect as it could be, he continued. The prognostic performance of nuclear cardiology is excellent. The new D-SPECT system (solid-state detector) may have better sensitivity and specificity because it has better spatial resolution, and examining time is reduced as well as greater accuracy. Conventional radiation exposure with thallium equals 20 mSv, with technetium that is reduced by approximately 50%. With rubidium the radiation exposure for rest and stress added together comes out at background level (approximately 3 mSv). Last year's guidelines from the U.K. National Institute for Health and Clinical Excellence recommend functional imaging for the intermediate-risk group.
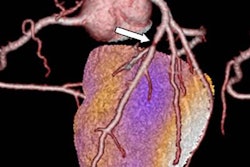
 PET/CT angiogram fusion image comprises a volumetric CT angiogram showing the structure of the heart and vessels in pink. A color flow map is superimposed on the left ventricle derived from the PET images. Gold is good myocardial blood flow, while purple is reduced flow. The combined imaging shows that distal to a LAD stent, there is flow limitation (purple color toward the apex of the left ventricle).
PET/CT angiogram fusion image comprises a volumetric CT angiogram showing the structure of the heart and vessels in pink. A color flow map is superimposed on the left ventricle derived from the PET images. Gold is good myocardial blood flow, while purple is reduced flow. The combined imaging shows that distal to a LAD stent, there is flow limitation (purple color toward the apex of the left ventricle).Hybrid imaging is a result of integrating nuclear cardiology with coronary CT angiography. It is achieved by combining flow, anatomical data, and nuclear cardiology, and is especially useful in detecting flow limitation, Groves explained. In nuclear cardiology, there is good (but not optimal) resolution. If it is necessary to double the spatial resolution, this means an increase of radiation exposure by a factor of four. Nevertheless, the benefits of combining nuclear cardiology with CT angiography means physiology is combined with anatomy; there is an improvement in diagnostic performance of CT angiography, and it is helpful to identify coronary calcifications and coronary stents and grafts.