Ultrasound combined with a novel computer-aided detection (CAD) scheme can help determine whether thyroid nodules are malignant or benign, a new study has found. The research team thinks it's feasible to identify malignant lesions, based primarily on the presence and patterns of thyroid nodule calcifications.
"Our results indicate that computerized ultrasound calcification features are statistically different between malignant and benign thyroid nodules," wrote Dr. Woo Jung Choi, Dr. Jeong Seon Park, and colleagues from Hanyang University and the University of Ulsan in Seoul, South Korea, and the National Cancer Center in Gyeonggi-do.
Calcifications are common findings in thyroid nodules that may or may not indicate malignancy, although they are more common in malignant lesions. Several studies have shown that the calcifications pattern is an important indicator of malignancy, with microcalcifications generally accepted as the most reliable indicator of malignancy, especially with regard to papillary carcinomas, the most common type.
As for macrocalcifications, they are more commonly found in malignant nodules than nonmalignant ones, but are not specific to thyroid cancer, the study team wrote (European Journal of Radiology, 25 June 2015).
Ultrasound is widely used as a diagnostic modality for thyroid nodules, revealing features commonly used for diagnosis such as shape, (for example, "taller than wide,") as well as speculated margins and hypoechogenicity.
Computer-aided analysis using ultrasound has recently gained ground as a diagnostic tool, using computer power to extract common features seen in the modality that can be used in diagnosis, the team wrote. But although ultrasound has been applied to evaluate textures from gray level histograms, extracting texture-based features from high-resolution or 3D images, it has not been used to analyze calcifications on thyroid nodules.
Indeed, CAD has not been applied to this task "despite the fact that calcifications have been shown to be common and valuable features that differentiate benign and malignant thyroid nodules," Choi et al wrote. "Therefore, we quantitatively assessed these features and determined their diagnostic performance in terms of ability to differentiate between malignant and benign thyroid nodules."
After excluding poor-quality images from a database of thyroid nodules acquired between 2004, and 2008, the study team evaluated 99 thyroid nodules (78 malignant and 21 benign) from 85 patients (61 women and 24 men; mean age, 52 years old; range, 29-81 years old) who underwent thyroid ultrasound followed by surgery within six months.
In all, 77 of the 78 cases found to be malignant by histology were papillary carcinomas, and the remaining case was a noninvasive follicular carcinoma. Two very experienced radiologists reviewed all of the cases.
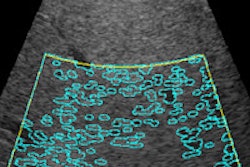
Computer analysis was applied to 147 images of 78 malignant nodules and 68 images of 21 benign nodules. First, the radiologists outlined the lesion boundary for each nodule using Image J software (National Institutes of Health). Then the authors' computerized analysis scheme was applied to quantitatively analyze the calcification features of each nodule.
Calcification features were extracted by semiautomatically segmenting calcifications using a nonparametric and unsupervised method for automatic threshold selection of image segmentation known as Otsu's algorithm.
The computerized analysis scheme was used to quantitatively analyze the ultrasound features of 99 pathologically determined calcified nodules. They used univariate analysis to identify features that were significantly associated with malignancy, then performed neural-network analysis to classify tumors as benign or malignant.
They applied receiver operating curve (ROC) analysis to evaluate the diagnostic performance of the algorithm, with the area under the curve (Az) applied to summarize the diagnostic performance of specific features, Choi and colleagues wrote.
Among all the newly described calcification features, the researchers chose four that reached statistical significance in the univariate analysis for use in the study, including:
- Ratio of calcification distance (calcification distance divided by the longest diameter, indicating calcification eccentricity) (0.80, p = 0.001)
- Numerical count of calcifications (0.68, p = 0.03)
- Skewness (asymmetry index of a calcification histogram) (0.82, p = 0.041)
- Maximum intensity (maximum echogenicity of the calcification) (0.75, p = 0.011).
Even so, the area under the ROC curve for the combined four features was, at 0.84, higher than that for any individual features above. Moreover, the researchers found no significant differences in diagnostic performance among any of the calcification features or combination thereof.
Aiming to assess the overall performance of the network, the group then examined the area under the ROC curve (Az) over the testing output values. At a threshold of 0.64, the Az value for the calcification features reached 0.83, with a sensitivity of 83%, specificity of 82.4%, and accuracy of 82.8%, Choi et al reported.
Benign, malignant statistically different
The results showed that ultrasound calcification features show statistically significant differences between malignant and benign thyroid nodules, the study team concluded.
"Even though there have been debates about the value of calcifications for distinguishing between malignant and benign calcifications, in our study, the ratio of calcification distance in benign thyroid nodules was larger than that for malignant nodules, which was consistent with the results of previous studies that concluded that peripherally located calcifications were typically benign."
Also in line with other recent reports, the study showed that malignant thyroid nodules had smaller numbers of calcifications, which were "dimmer" than those of benign nodules. They added that specimen radiography continues to be a useful tool for diagnosing cancer type and predicting cancer extent.
Computerized analysis has natural advantages over manual methods, principally in its ability to "reveal complex relationships between different input variables that are often very difficult to determine using conventional statistical methods," Choi et al wrote. Even though the calcification features and combined features did not show significant differences in performance, the combined features remained the strongest predictor.
The diagnostic performance of the neural network estimated from the area under the ROC curve "suggest that there is potential to reduce operator dependency in the interpretation of calcified thyroid nodules, which may improve the consistency of radiological diagnoses," they wrote.
"The results .... support the use of computerized analysis for differentiating between malignant and benign calcified thyroid nodules, despite several shortcomings of this method," they added.
Limitations included the use of 2D data, and the inclusion of only surgery-proven cases, which had the effect of excluding clinically observable benign nodules, and may therefore have introduced selection bias.
The diagnostic performance of the program was particularly useful for differentiating calcified nodules as malignant or benign, they wrote.
"Our results show that malignant thyroid nodules have shorter calcification distance ratios, smaller numbers of calcifications, and dimmer calcifications," Choi et al wrote. "The computerized analysis of malignancy probability in a given calcified thyroid nodule could potentially be used to establish probabilistic thresholds for treatment decisions, including fine needle aspiration and extended medical management."