Less-motion-sensitive T2-weighted BLADE -- Siemens Healthcare's proprietary name for a turbo spin-echo (TSE) sequence to acquire multiple echo trains -- should not replace conventional TSE when imaging a woman's pelvis because, despite its appeal, overall contrast suffers, according to Swiss researchers.
T2-weighted contrast imaging has been proposed as part of a basic MRI protocol for workup of pathologies of a woman's genital organs, such as sonographically indeterminate adnexal masses or staging of endometrial cancer with MRI. In pelvic MRI, respiration, cardiac motion, and intestinal peristalsis often produce movement or ghosting artifacts that may result in poorly defined organ contours and reduced detection of pathological lesions. There have been many proposals to solve the limitations, but they don't work in the clinical routine.
The multiple oversampling of central k-space using periodically rotated overlapping parallel lines with enhanced reconstruction (PROPELLER) offers advantages over other methods for patient motion correction, as it corrects for two types of motion: in-plane rotation and translation. Unlike rectilinear k-space sampling, BLADE uses a TSE sequence to acquire multiple echo trains in a rotating, partially overlapping fashion.
"This technique is less susceptible not only to bulk motion but also to flow-related artifacts from vessels, and has been evaluated for replacing sequences with conventional Cartesian k-space acquisition in the brain," wrote Dr. Johannes Froehlich, from the department of radiology at Kantonsspital Baden in Switzerland, and colleagues (Insights into Imaging, 26 September 2012, online first).

 The uterine zonal anatomy and cervix are more sharply delineated on the BLADE image (right); however, SNR and CNR are higher on the conventional T2-weighted image (left). All images courtesy of Dr. Bianka Freiwald-Chilla.
The uterine zonal anatomy and cervix are more sharply delineated on the BLADE image (right); however, SNR and CNR are higher on the conventional T2-weighted image (left). All images courtesy of Dr. Bianka Freiwald-Chilla.Previous studies have focused primarily on visual and qualitative assessment of images, so Froehlich and colleagues prospectively compared overall image quality, contrast, and diagnostic information of the recently implemented T2-weighted BLADE TSE sequence with the conventional Cartesian T2-weighted TSE sequence in female pelvic organs.
They found BLADE significantly (p < 0.0001) reduced motion and ghosting artifacts and showed improved conspicuity, but overall image quality did not differ significantly in the 47 patients who underwent sagittal BLADE and conventional TSE at 1.5-tesla after glucagon administration. In the majority of cases (53.2% versus 59.6%), radiologists preferred conventional TSE due to better image contrast and visibility of free pelvic fluid. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were significantly higher on conventional TSE.
"In our comparative study, the overall image contrast was reduced when using BLADE. This might be explained with the nonuniform T2-weighting along the width of the blade, i.e., the phase-encoding direction with contrast predominantly determined by low-frequency data as described by Pandit et al," Froehlich and colleagues wrote. "The reduced SNR and CNR in BLADE images occurred despite more frequent sampling of the k-space center. This was likely because the bandwidth in BLADE was twice as large as in conventional TSE (260 Hz per pixel in BLADE compared with 130 Hz per pixel in conventional TSE)."
There was also a lower angle used in BLADE (145°) compared with conventional TSE (170°) for the radiofrequency refocusing pulses in the TSE echo train, which may have resulted in reduced signal and T2-weighting in the BLADE images.

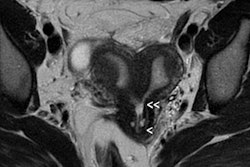
 Cervical carcinoma: The uterine zonal anatomy and bladder wall as well as the bowel loops are more sharply delineated on the BLADE image (right); however, SNR and CNR are higher on the conventional T2-weighted image (left).
Cervical carcinoma: The uterine zonal anatomy and bladder wall as well as the bowel loops are more sharply delineated on the BLADE image (right); however, SNR and CNR are higher on the conventional T2-weighted image (left)."Indeed, conventional T2-weighted TSE provided a significantly better visibility of free pelvic fluid or cystic structures (i.e., a relatively higher effective T2 weighting) in numerous cases," the researchers noted.
Both radiologists involved in the study preferred T2-weighted conventional sequences, despite the reduction of movement and ghosting artifacts provided by BLADE.
"This may be related to the importance of the presence of free fluid in the pelvis as an important early sign of infection, trauma, carcinomatosis, or inflammation. The readers' preference for conventional TSE suggests that, in addition to the reduction of motion artifacts, image contrast must also be considered when developing BLADE protocols for female pelvic MRI," the researchers wrote.
BLADE improves anatomic depiction and image quality thanks to less movement artifact, but at the expense of CNR of cystic structures or visibility of free pelvic fluid.

 Adenomyosis and intramural leiomyomas: The intramural uterine changes, cervical structures, and bladder wall are more sharply delineated on the BLADE sequence (right); however, SNR and CNR are higher on the conventional T2-weighted image (left). There are also fewer motion artifacts in the surrounding tissue on the BLADE image.
Adenomyosis and intramural leiomyomas: The intramural uterine changes, cervical structures, and bladder wall are more sharply delineated on the BLADE sequence (right); however, SNR and CNR are higher on the conventional T2-weighted image (left). There are also fewer motion artifacts in the surrounding tissue on the BLADE image."From a diagnostic point of view, the distinctive MRI properties of cystic structures are of primary importance when performing female pelvic imaging," they added. "Additional use of contrast showing enhancement of solid tumor components besides including conventional non-Cartesian sampled T1- and T2-weighted images into the protocol are advocated to facilitate the diagnosis and to avoid pitfalls."
The researchers also state in a clinical setting, the prolonged reconstruction time of BLADE is a practical drawback which must be considered. Postprocessing times are dependent on the size of the raw data and are influenced by technical parameters such as blade width, coverage or parallel imaging factors, and duration of the motion correction algorithm.
The study had some limitations:
- It focused on qualitative and quantitative criteria describing and analyzing image quality and contrast parameters.
- The differing sequence parameters such as the differing bandwidth, flip-angle, voxel sizes, and echo time values of the two pulse sequences may be a limitation when comparing SNR and CNR values.
- The slightly shorter echo time of BLADE (86 msec compared with 101 msec for conventional TSE) does not appear to explain the quantitative contrast differences encountered.
- They did not evaluate the performance of BLADE without the use of an antiperistaltic agent for clinical reasons.
BLADE may be useful in selected cases with uterine pathologies and in cases where severe motion artifacts may be problematic using conventional T2-weighted pulse sequences. "However, due to the issues described, we would not currently recommend general replacement of conventional T2-weighted TSE sequences by BLADE in the female pelvis," the authors concluded.
The authors acknowledged this study was in part supported by a research grant from Guerbet Switzerland. They maintained full control of the design of the study, collection, analysis and interpretation of data, content, and writing of the manuscript. There is no conflict of interest concerning the funding of this study and the addressed subject, they wrote. One of the co-authors, Markus Klarhöfer, is an employee at Siemens and provided support for the used sequences, but did not interfere in either patient selection or the image interpretation process.