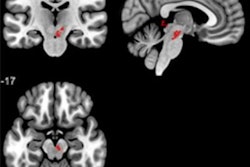
Susceptibility-weighted MR imaging (SWI) is a viable alternative to perfusion-weighted MR imaging (PWI) to assess reduced blood flow and predict stroke evolution, according to a study published online on 10 February in European Radiology.
The benefit of SWI in stroke cases is that the technique does not require a contrast agent, as PWI does, thus making SWI a potentially much more viable option for patients in general, and particularly those who are adverse to contrast agents due to renal insufficiency and previous allergic reactions.
Lead study author was Dr. Hung-Wen Kao from the Irvine Medical Center in Irvine, California.
As the authors noted, therapy for acute ischemic stroke targets the area of reduced blood flow but to such a degree that it can cause irreversible cell membrane failure. While it has limitations, Kao and colleagues wrote that a "mismatch between larger abnormal areas on PWI and smaller restricted areas on diffusion-weighted imaging (DWI) is a widely accepted approach to detecting penumbra (reduced blood flow), predicting stroke evolution, and determining patients with the greatest potential to benefit from thrombolytic therapy."
SWI offers a high-resolution, 3D, gradient-echo MRI technique, which can display blood characteristics, iron, and calcifications. Traditionally, SWI has been used in trauma cases, vascular malformations, tumors, and cerebrovascular and neurodegenerative diseases.
Study population
Researchers retrospectively culled data from 303 consecutive patients with acute stroke between January 2009 and September 2010. The study sample included patients who, among other factors, received MRI exams within 24 hours of stroke symptom onset and follow-up MRI or CT exams at least five days later to assess the size of any infarctions.
A total of 19 patients met the inclusion criteria, but four patents developed hemorrhages on follow-up studies, leaving 15 patients (seven women, eight men; median age of 68 years; range 35-89) for the study sample.
MRI exams were performed with a 1.5-tesla system (Magnetom Avanto, Siemens Healthcare) with a 12-channel head coil. Acquired images included DWI and SWI, as well as PWI after injection of a gadolinium-based contrast agent (Omniscan, GE Healthcare). Follow-up CT images were acquired using a 64-slice scanner (Somatom Sensation 64, Siemens) with a slice thickness of 5 mm.
Researchers also used a 10-point CT scoring system, known as the Alberta Stroke Program Early CT Score (ASPECTS) to assess the size of any abnormal signal intensities or densities on individual DWI, SWI, PWI, and final infarct studies.
Image evaluations
Two neuroradiologists who were blinded to patient information except for the clinical history of ischemic stroke, independently assessed ASPECTS values on the selected images. To determine the values, one point was subtracted from 10 for an area of ischemic changes, which included factors such as restricted diffusion, reduced relative cerebral blood flow, and relative cerebral blood volume.
Researchers also divided the subjects into two groups. Six patients that showed infarct growth were placed into one group, while the remaining nine patients were in the group that showed no infarct growth.
Final infarct studies were obtained at a median of seven days after stroke symptom onset.
A total of 10 patients (67%) received follow-up CT scans, while five individuals (33%) were given MRI exams. The results found cerebral ischemic infarcts in the area of the right middle cerebral artery in seven patients (47%) and in the left middle cerebral artery in eight patients (53%).
In addition, SWI discovered blood clots, or thrombi, which caused the infarcts in 14 patients (93%). The images showed 13 thrombi (93%) in one segment of the middle cerebral artery and one thrombus in another artery segment.
SWI-DWI correlation
Researchers also found the correlation between SWI and DWI was significantly associated with the infarct growth group, and the difference between the abilities of SWI and DWI to predict infarct growth was 6.7%.
"ASPECTS values on initial DWI, SWI, and PWI were significantly correlated with those on follow-up studies, but not associated with infarct growth," the authors wrote.
Kao and colleagues noted several limitations of their study, including the few patients in the sample. They also noted ASPECTS values on the imaging parameters with p < 0.05 should be considered "marginally significant" given the small patient population.
The researchers also recommended follow-up prospective studies to evaluate the role of SWI in guiding thrombolytic therapy.
Editor's note: The thumbnail on our homepage is of a 58-year-old man who experienced a vertebrobasilar stroke. The MR coronal fluid-attenuated inversion-recovery (FLAIR) image shows multiple ischemic lesions in vertebrobasilar territory. Image courtesy of Dr. Luca Valvassori and Dr. Mariangela Piano, from the department of neuroradiology, Ospedale Niguarda Ca'Granda, Milan, Italy.