Seat-belt injuries resulting from trauma in road traffic accidents can be misdiagnosed initially, and they may be life-threatening and require surgical intervention. Great care must be taken with vascular bowel and mesenteric injuries, radiologists from Spain have reported.
"It is key for the reading radiologist of a CT during the evaluation of patients with seat-belt injuries to know the typical patterns of these lesions," noted Dr. Eric Castañé Isern, a third-year radiology trainee, and colleagues from the Hospital Universitario 12 de Octubre in Madrid.
Seat belts reduce mortality and morbidity rates, but during high deceleration, they generate shearing forces and compressive effects, causing specific injuries, the team told ECR 2023 delegates. "Lumbar hernias are highly associated with intraabdominal injuries. Major abdominal vascular injuries are seen frequently, especially the small intimal flaps, which can be treated conservatively."
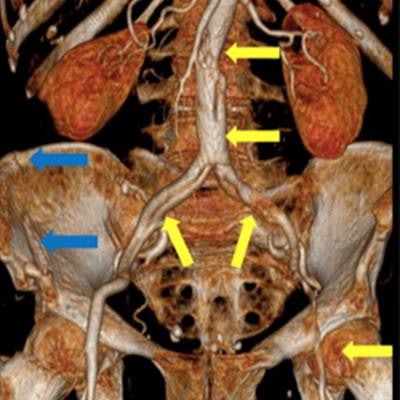
 Seat-belt aorta. 3D maximum intensity projection reformation (A) and vascular 3D reformation (B) of a patient with abdominal aortic dissection. The beginning of the dissection is in the L3-L4 level, which is typical in a case of seat-belt aorta. It extends until the left femoral artery. There was also a pelvic ring fracture (blue arrows). All figures courtesy of Hospital Universitario 12 de Octubre and presented at ECR 2023.
Seat-belt aorta. 3D maximum intensity projection reformation (A) and vascular 3D reformation (B) of a patient with abdominal aortic dissection. The beginning of the dissection is in the L3-L4 level, which is typical in a case of seat-belt aorta. It extends until the left femoral artery. There was also a pelvic ring fracture (blue arrows). All figures courtesy of Hospital Universitario 12 de Octubre and presented at ECR 2023.The group reviewed CT images of traffic accidents with clinical evidence of seat-belt injuries (anatomic abdominal injury, thoracic injury, and other injuries) from an internal trauma database of 81 patients built up since 2010. This database also includes demographic data, the mechanism of the motor vehicle collision, and clinical outcomes.
Types of injuries
The seat-belt sign consists of the skin contusion from the seat belt seen in the lower abdomen wall, chest wall, breast, and neck, the group stated in a poster.
Classically, the "seat-belt syndrome" consisted of the combination of soft-tissue injuries plus internal visceral or spinal injuries. Soft-tissue ecchymosis is a guide sign visible also on CT and should alert the radiologist for the presence of internal injuries, especially if the ecchymosis is above the line between the two anterior superior iliac spines, indicating a mispositioning of the lap belt.
"The soft tissue ecchymosis caused by the shoulder harness can be found through the chest wall, the breast, and the neck," the authors wrote. "Blunt cerebrovascular injury is uncommon. Carotid blunt trauma has been reported. The vertebral arteries can also be involved, especially if a fracture of the transverse foramen up to C7 is present."
A cervical seat-belt sign does not necessarily increase the risk of vascular damage, they continued. Some authors suggest that in the absence of other clinical findings, the seat-belt sign does not independently justify neck CT angiography, but the guidelines adopt a liberal approach. "In a multi-institutional study, it is recommended vascular examination in the presence of at least one additional traumatic finding to the head, neck, and upper chest or a new neurological deficit."
 Blunt cerebrovascular injury. Patient after a motor vehicle collision and with seat belt sign. On initial CT exam, a right cervical hematoma (A) and first left rib fracture (B) were seen. The neck CT scan revealed a right carotid dissection. Angiography (D) shows the dissection (yellow arrow) and a superior segment with stenosis due to a subintimal hematoma (red arrow), and a pseudoaneurysm (red circle).
Blunt cerebrovascular injury. Patient after a motor vehicle collision and with seat belt sign. On initial CT exam, a right cervical hematoma (A) and first left rib fracture (B) were seen. The neck CT scan revealed a right carotid dissection. Angiography (D) shows the dissection (yellow arrow) and a superior segment with stenosis due to a subintimal hematoma (red arrow), and a pseudoaneurysm (red circle).Cervical spine injuries occur because of the oblique hyperflexion and the following hyperextension leading to ligamentous cervical injuries, which are better assessed with an MRI. The thyroid gland can also be injured by compression forces, causing a hematoma with the underlying risk of airway obstruction, requiring urgent thyroidectomy.
"Other head and neck injuries reported are cervical laryngotracheal injuries and cervical esophagus lesions (rare). These injuries are caused by compressive and rotational forces of the shoulder harness against the cervical aerodigestive tract," the researchers pointed out.
Chest wall injuries tend to align along the axis of the belt. Ribs and sternal fractures are the most common chest wall fractures, but clavicles can also be involved. Sternal fracture is better seen in the sagittal plane and the underlying anterior mediastinal hematoma is better assessed in the axial plane, and fractures of the chondrocostal union are better seen with a soft-tissue window, they stated.
Although rare, breast implant ruptures may occur. These and soft tissue injuries of the chest wall are more frequent when the shoulder harness does not lay over osseous structures.
 Chest wall injury. (A-D) show a patient with breast hematoma with active bleeding (yellow arrows), with mass effect over the right breast implant. Note the implant's surface in C (blue arrows) and D (3D reformation). (E) Breast implant rupture and an underlying rib fracture (blue circle).
Chest wall injury. (A-D) show a patient with breast hematoma with active bleeding (yellow arrows), with mass effect over the right breast implant. Note the implant's surface in C (blue arrows) and D (3D reformation). (E) Breast implant rupture and an underlying rib fracture (blue circle).Fractures of the chest wall are often accompanied by lung contusions and hemopneumothorax. In severe collisions, thoracic aortic rupture through the isthmus or dissection can occur. Other types of intimal injuries are pseudoaneurysms or intimal defects with no aortic contour abnormality.
"Diaphragmatic ruptures are caused by the mispositioning of the lap belt, the sliding of the occupant under the belt during the impact, and the high increase in the intraabdominal pressure," the authors wrote. "They are better assessed in the coronal plane, and fractures or angulation of the ribs and subcutaneous emphysema can be clues."
Abdominal wall hernias occur because of the shearing forces through the myofascial layers of the abdominal wall during the sudden deacceleration and the high increase in the intraabdominal pressure. They occur through the weakest anatomical sites of the abdominal musculature. Multiplanar reformation should be performed to increase sensibility.
"Although they are misdiagnosed clinically, their presence indicates the violence of the accident and they are associated with a high risk of surgical intraabdominal injuries; either herniated intraabdominal structures or structures far from the herniation site," they explained. "Other abdominal wall injuries include soft tissue contusion or direct muscle rupture."
Bowel and mesenteric injuries
In motor vehicle collisions bowel injuries are more likely to be ischemic than in other blunt trauma or penetrating trauma, the researchers continued.
"They occur because of shearing forces at the junction of mobile and fixed bowel plus the high intraabdominal pressure caused by the entrapment of intestine loops over and above the lap belt," they pointed out. "These mechanisms can cause a bucket-handle tear which is an injury in which the mesentery avulses off a bowel loop. Mesenteric injury can be misdiagnosed first causing a delay in surgical intervention."
These kinds of ischemic injuries are more frequent in the ileocecal region and proximal jejunum. In the Madrid facility's database, the small intestine was damaged more frequently than the colon.
 Bowel and mesenteric injury. CT signs of bowel damage consisting of pneumoperitoneum (blue arrow in B) and mesenteric damage consisting of hemoperitoneum and active bleeding (yellow arrow). There is also hypoenhancement of ileal loops (white arrow). Note the subcutaneous fat stranding (red arrow in A).
Bowel and mesenteric injury. CT signs of bowel damage consisting of pneumoperitoneum (blue arrow in B) and mesenteric damage consisting of hemoperitoneum and active bleeding (yellow arrow). There is also hypoenhancement of ileal loops (white arrow). Note the subcutaneous fat stranding (red arrow in A).The most specific CT signs are bowel mural discontinuity, pneumoperitoneum, or active mesenteric bleeding.
"Free oral contrast is considered by some authors as the most specific sign of blunt trauma of the bowel and mesentery," they wrote. "Nevertheless, a retrospective single-center study found that hyperenhancement of the bowel adjacent to a hypoenhancing segment would be the most specific sign in a routine trauma CT exam."
Free fluid or interloop fluid, bowel wall thickening, or mesenteric contusions are relatively less specific signs, but they are more prevalent, according to the authors.
To view the whole ECR 2023 poster and learn more about the full range of cases, go to the EPOS section of the congress organizers' website.
The co-authors of the ECR e-poster were Lain Ibañez Sanz, Sara Munck Sánchez, Paula Heredia Cachá, Beatriz Bermejo Guerrero, Maria Elena Martínez Chamorro, Estefania Aguilar Angel, Carlos García Fuentes, and Susana Borruel Nacenta



















