MRI is proving to be an excellent tool when investigating deaths of unknown origin that are inconclusive at either postmortem or histological examination. Also, the use of extended scale CT for identification purposes is proving exciting when visual identification alone is not possible due to disfiguration or decomposition of the body.
 It could take another 10 to 20 years before 3-tesla MRI is used widely in forensic postmortem, according to Dr. Christian Jackowski.
It could take another 10 to 20 years before 3-tesla MRI is used widely in forensic postmortem, according to Dr. Christian Jackowski.At the Institute of Legal Medicine in Zurich, which deals with all types of unnatural death including shootings and stabbings, human remains are routinely imaged in submillimeter resolution with CT. Scan speed is less an issue than the need for a wide gantry for burn victims, which often present in splayed position. In addition, extended scale CT can help locate and characterize foreign bodies such as bullets, knife tips, screws, or catheters aiding in optimal postmortem planning.
"While the clinician wants to reduce artifacts to get a clear image of the tissue around a foreign body, we reduce them to see the object itself," said Dr. Christian Jackowski, who specializes in CT and MR postmortem examinations.
A case in point is the visualization of dental fillings. Dental x-ray plays a key role alongside DNA in identifying human remains whether in mass fatalities or single incidents when bodies have undergone alteration after death. Up to 80% of postmortem identification in the wake of the Asian tsunami in 2004 was based on dental status. Ultrahigh-resolution dual-source CT with extended CT scale has proved to reduce streak-induced artifacts and distinguish between fillings, whether composite, amalgam, ceramic, or temporary fillings, based on radiopacity in Hounsfield units, their size, and location.
 Cross section of investigated teeth and Hounsfield unit profile along a measurement indicated as a white line in the molar. All images courtesy of Dr. Christian Jackowski.
Cross section of investigated teeth and Hounsfield unit profile along a measurement indicated as a white line in the molar. All images courtesy of Dr. Christian Jackowski. A volume rendering preset suggestion to apply for dental CT data based on the investigated teeth. White for physiological dental structures such as dentine and enamel. Low opaque composite fillings are shown in green whereas high opaque composite fillings are shown in red.
A volume rendering preset suggestion to apply for dental CT data based on the investigated teeth. White for physiological dental structures such as dentine and enamel. Low opaque composite fillings are shown in green whereas high opaque composite fillings are shown in red.Using a Siemens Healthcare Definition Flash, Jackowski has dedicated the past year of ongoing research to the development of a dual-energy application of more than 30,000 Hounsfield units and a software tool to analyze the data obtained to further characterize filling materials. This development could have implications for other areas of postmortem imaging such as bullet characterization.
Soft-tissue visualization of postmortem CT is outclassed by MRI, and although there are no patient-related scan time limits, time is still an issue in criminal investigations such as hit-and-runs. Given that an MR scan can take an extra two to five hours after a CT exam, careful selection of cases in which MR can substantiate CT, or even provide additional information, is paramount, particularly when police are waiting for results before pursuing a line of inquiry or even a suspect.
"From the MR point of view, a gunshot to the head is less interesting. With MRI, the gunshot channel is comparably seen as in autopsy, but for pedestrians killed by cars, MR sometimes detects more lesions than autopsy and in sudden cardiac deaths even more than histology can," he said.
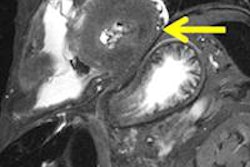
 Chronic myocardial infarction in postmortem MRI (death occurred months to years after infarction). A T2-weighted short axis image depicts a severe shrinking of the lateral wall with broad decrease of signal (arrow). Autopsy demonstrated definite collagenous transformation of the infarcted inferior myocardium with scar-caused shrinking (not shown). Histology (H&E) showed cell-free collagen formation as the cause for the significant decrease of signal in MRI.
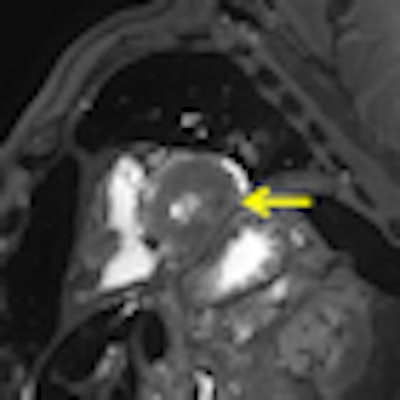
Chronic myocardial infarction in postmortem MRI (death occurred months to years after infarction). A T2-weighted short axis image depicts a severe shrinking of the lateral wall with broad decrease of signal (arrow). Autopsy demonstrated definite collagenous transformation of the infarcted inferior myocardium with scar-caused shrinking (not shown). Histology (H&E) showed cell-free collagen formation as the cause for the significant decrease of signal in MRI. Acute myocardial infarction in postmortem MRI (death occurred after two to three days). A T2-weighted short axis image demonstrates a hypointensity with surrounding edema within the lateral wall. Autopsy revealed a yellowish alteration at the same location (not shown). Histology demonstrated early granulocyteous infiltration (not shown).
Acute myocardial infarction in postmortem MRI (death occurred after two to three days). A T2-weighted short axis image demonstrates a hypointensity with surrounding edema within the lateral wall. Autopsy revealed a yellowish alteration at the same location (not shown). Histology demonstrated early granulocyteous infiltration (not shown). Peracute myocardial infarction in postmortem MRI (death occurred after minutes to one hour). A T2-weighted short axis image presents with a local hypointensity within the lateral wall without hyperintense edematous margin. Autopsy aspect of the specimen showed no visible alteration within the affected myocardium (not shown). Histology also failed in demonstrating ischemic alterations (not shown). Dissection of the coronary artery system revealed a fresh soft plaque rupture with intimal hemorrhage within the circumflex coronary artery (not shown).
Peracute myocardial infarction in postmortem MRI (death occurred after minutes to one hour). A T2-weighted short axis image presents with a local hypointensity within the lateral wall without hyperintense edematous margin. Autopsy aspect of the specimen showed no visible alteration within the affected myocardium (not shown). Histology also failed in demonstrating ischemic alterations (not shown). Dissection of the coronary artery system revealed a fresh soft plaque rupture with intimal hemorrhage within the circumflex coronary artery (not shown).Sudden cardiac death happens mainly due to ventricular tachycardia with no direct findings in the heart in autopsy or histology as speed of death leaves insufficient time for recognizable myocardial changes. Jackowski's most recently published study demonstrates that unenhanced MR can show peracute myocardial infarctions even in the absence of a myocardial autopsy finding, and when histology may fail to show ischemic alterations.
Postmortem MRI may bridge the gap caused by declining autopsy rates. However, given the different sequences needed for the varying body temperatures of corpses and the restricted predefined scan area required, the postmortem doctor is challenged by time spent versus quality achieved.
Efforts to adapt clinical MR sequences to postmortem applications through quantitative MR scanning protocols started in 2007 and were boosted in September 2010 by the addition of a Philips Healthcare 3-tesla MR unit to the project, making Zurich the only forensic institute to use 3 tesla in routine MRI for selected cases. It could be another 10 to 20 years before 3-tesla MRI becomes a more widespread forensic postmortem application, according to Jackowski.